Yes — often curable when found early. Dr. Lucas Minig explains stages, treatments, and what to expect in Spain. Book a specialist consultation today.
Introduction
Endometrial (uterine) cancer is a diagnosis that raises immediate questions: “Can it be cured?” and “What are my next steps?” This detailed guide answers those questions clearly, uses Spain-specific data and practice patterns, and explains why early action and the right doctor matter.
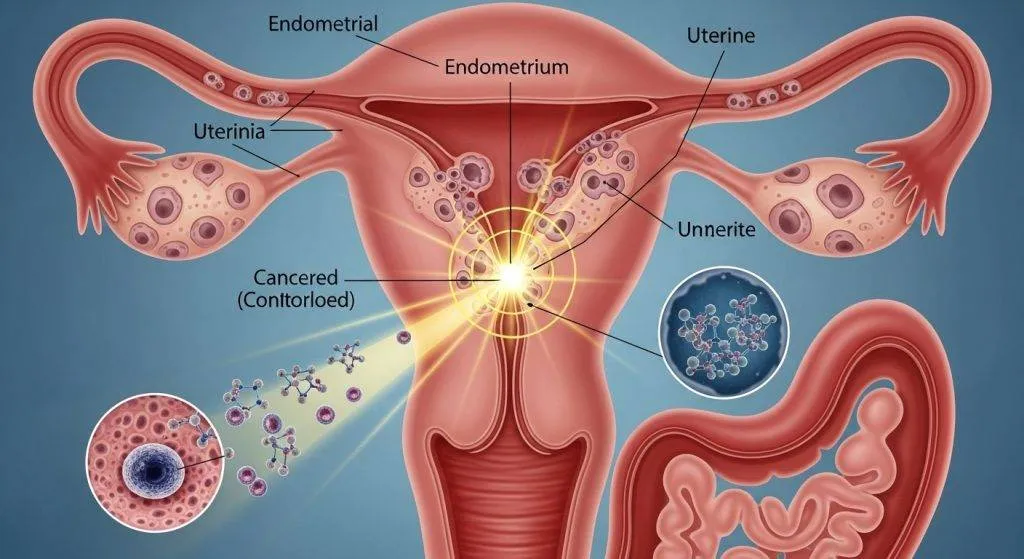
What is endometrial (uterine) cancer?
Endometrial cancer starts in the lining of the uterus (the endometrium). It most often presents with abnormal vaginal bleeding — a symptom that frequently leads to early diagnosis and, consequently, better outcomes in many patients.
Endometrioid vs. aggressive subtypes
Endometrial cancer is not a single disease. The most common form, endometrioid carcinoma, tends to grow relatively slowly and is usually hormone-sensitive. Other subtypes (serous, clear-cell, and some high-grade forms) are biologically more aggressive and behave differently in terms of spread and responsiveness to standard therapies. These differences strongly influence treatment decisions and prognosis.
Is Endometrial Cancer Curable?
In many cases, yes — especially when diagnosed at an early stage. Modern surgery and tailored adjuvant therapy cure (endometrial cancer) a large proportion of patients; for others, newer targeted and immune therapies can meaningfully extend survival and quality of life.
What “curable” means for cancer patients?
“Curable” means the treating team believes the cancer can be eradicated such that it will not return — the goal most often achieved when disease is localized and removed completely (for endometrial cancer, typically by surgery).
Why timing matters?: stage, grade, and biology
Three features determine most of the prognosis: how far the tumor has spread (stage), how abnormal the cells look (grade), and the tumor’s molecular profile (for example, mismatch repair deficiency or POLE mutations). Early stage + low grade + favourable molecular features = much higher likelihood of cure.
Why stage matters: the single biggest factor?
Stage is the clearest predictor of outcome — the earlier the stage at diagnosis, the higher the chance of cure. That’s why symptom awareness and prompt evaluation in Spain (or anywhere) are crucial.
Stage I, II, III, IV — what they mean
- Stage I: Tumor confined to the uterus.
- Stage II: Tumor reaches the cervix but is still within the uterus/cervix region.
- Stage III: Local spread to nearby tissues or regional lymph nodes.
- Stage IV: Distant spread to organs such as the bladder, bowel, liver, or lungs.
(Updated FIGO staging incorporates histology and molecular data to refine prognosis and treatment planning.)
Typical 5-year survival benchmarks
Survival varies by stage and by series, but approximate benchmarks used in clinical counseling are: localized disease often yields 5-year survival rates in the 80–95% range, regional disease lower (commonly 50–75% depending on risk factors), and distant metastatic disease with much lower 5-year survival (often around or below 20% in many cohorts for recurrent/advanced cases). These figures reflect aggregated international and Spanish data.
Cure Rates by Stage
- Stage I – Cancer Confined to the Uterus: This is the most curable scenario. Standard treatment — hysterectomy with removal of ovaries and appropriate lymph-node assessment — cures the majority of patients diagnosed at this stage; many centers report very high 5-year survival for stage I disease.
- Stage II – Spread to the Cervix: Cure is still a realistic aim but often requires more extensive surgery and sometimes adjuvant radiation or chemotherapy depending on pathology.
- Stage III – Local or Lymph Node Spread: Here treatment is multimodal (surgery plus adjuvant chemoradiation in many cases). Cure is possible, but outcomes are more variable and depend on how much disease can be removed surgically and the tumor’s biology.
- Stage IV – Advanced or Metastatic Disease: When the cancer has metastasised, long-term cure is uncommon, but some patients achieve durable responses with systemic therapy, targeted agents and immunotherapy—particularly if their tumor has actionable molecular features. Clinical trials and specialized care in major Spanish oncology centers can open additional options.
How doctors decide whether it’s curable?
After diagnosis, a team of specialists assesses imaging, pathology and molecular markers to determine stage and the most effective curative strategy.
Staging and the FIGO system (simple explanation)
FIGO staging (the international standard) combines clinical, surgical, and pathological information to place a case into stage categories that guide treatment. Newer FIGO updates emphasize molecular classification to improve prognostic accuracy.
Tumor grade and histology — what they tell us
Pathology describes both grade (cellular appearance/aggressiveness) and histologic type (endometrioid, serous, clear-cell, etc.). High-grade histologies and serous/clear-cell types tend to act more aggressively and have a higher recurrence risk; that affects decisions about adjuvant therapy.
Molecular subtypes (MSI / MMR, POLE, serous)
Molecular testing—identifying mismatch repair deficiency (MMRd)/microsatellite instability (MSI), POLE mutations, and p53 abnormalities—helps predict prognosis and guide the use of immunotherapy or other targeted treatments. For example, patients with MMRd tumors may respond especially well to checkpoint inhibitors.
Survival Rates and Prognosis in Spain
Spain has high-quality cancer services; survival for localized endometrial cancer is favorable, but national trends show nuances and ongoing need for early diagnosis and optimized care pathways.
Spain statistics in brief: national and regional studies indicate that 5-year survival for localized uterine cancer is generally high (often >80%), but some reports show a plateau or small decline in net survival in recent years, underscoring the need for ongoing attention to risk factors and access to care.
How healthcare quality impacts outcomes?
Access to multidisciplinary teams, prompt biopsy and imaging, and availability of specialized surgery (minimally invasive and sentinel node techniques) all improve outcomes. Spain’s major centers (university hospitals and oncology institutes) lead in implementing these standards.
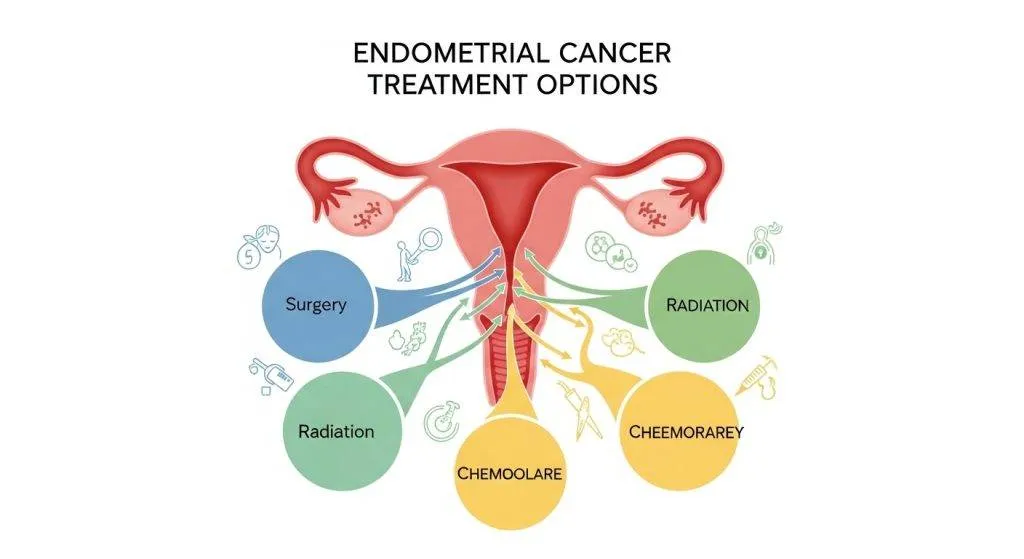
Treatments That Make Endometrial Cancer Curable
Early detection followed by the appropriate combination of surgery, radiation and systemic therapy is the route to cure in many patients.
Surgery (Hysterectomy)
Removing the uterus (hysterectomy) with surgical staging remains the foundation of curative treatment for most endometrial cancers. The surgical specimen provides essential information that determines the need for other treatments.
Minimally Invasive and Robotic Surgery
Where appropriate, laparoscopy or robotic surgery reduces recovery time and surgical morbidity while permitting accurate staging — an approach widely used in Spanish specialist centers and in expert practices such as the Valencia clinic led by Dr. Minig, which emphasizes minimally invasive techniques for eligible patients.
Radiation Therapy
Radiation (external beam and/or vaginal brachytherapy) lowers local recurrence risk in selected patients and is an important adjuvant tool after surgery for intermediate- or high-risk pathology.
Chemotherapy
Systemic chemotherapy (commonly carboplatin + paclitaxel) is used when the risk of distant recurrence is significant—either after surgery for high-risk cases or as primary therapy in advanced disease.
Immunotherapy and Targeted Therapy
Checkpoint inhibitors and other targeted drugs have changed the landscape for recurrent or metastatic disease, particularly for tumors with MSI/MMRd or other actionable alterations. Spain’s research centers and oncology programs actively trial and apply these therapies for selected patients.
Fertility-sparing and special cases
Some younger patients want to preserve fertility — in carefully selected situations this is possible under strict surveillance.
Who can avoid hysterectomy?
Women with very early, low-grade, endometrioid tumors and no myometrial invasion may be candidates for progestin-based therapy and close follow-up instead of immediate hysterectomy — but this requires detailed counseling and expert center management.
What do doctors in Spain do for younger patients?
Spanish gynecologic oncology teams offer fertility-preserving protocols at specialized centers; these programs pair medical management with close biopsy and imaging follow-up to catch progression early. Consultation with a specialist (for example, an experienced gynecologic oncologist in Valencia) is recommended to evaluate eligibility and risks.
When is cure less likely? — realistic, compassionate talk
Honest communication about prognosis is essential. If disease is metastatic, cure becomes an uncommon goal, but individualized treatments can still provide meaningful control and symptom relief.
Advanced/metastatic disease and long-term control
For selected patients, systemic therapy and targeted approaches can produce durable responses; enrollment in clinical trials at major Spanish centers is often an important option.
Palliative care vs. curative intent
Palliative care should be integrated early when cure is unlikely — it focuses on symptom control and preserving quality of life while other cancer-directed therapies may continue.
Recurrence: What If the Cancer Comes Back?
Recurrence can be local, regional, or distant. Management depends on previous treatments and the site of recurrence — salvage surgery, radiotherapy, chemotherapy, or immunotherapy (when indicated) can provide further disease control and sometimes long-term survival. Early detection of recurrence improves options.
Factors That Improve the Chances of Cure
- Early diagnosis prompted by symptom awareness (e.g., post-menopausal bleeding).
- Care at multidisciplinary centers with gynecologic oncologists, pathologists and radiation/medical oncology teams.
- Access to minimally invasive surgery and sentinel node techniques.
- Molecular testing that opens targeted/immunotherapy options.
- Rapid pathways for evaluation and treatment — many Spanish centers and specialist clinics provide expedited workups.
When Is Endometrial Cancer Not Curable?
Cure is unlikely when disease is widely metastatic and not amenable to complete surgical removal, or when tumor biology is highly aggressive and non-responsive to available systemic therapies. Even then, effective palliative therapies can control symptoms and extend survival.
Meet the clinician: Dr Lucas Minig
Training and approach: what sets his care apart
Dr. Lucas Minig combines fellowship-level training in minimally invasive gynecologic oncology with experience in multidisciplinary care and international practice. He emphasizes precision surgery (often minimally invasive), rapid diagnostic pathways, and personalized treatment planning — all factors that can enhance the likelihood of curative outcomes for eligible patients. See his clinic’s quick-access model for fast workups in Valencia.
What to expect at a consultation in Spain
A typical consultation with a specialist like Dr. Minig includes a focused history, review of pathology and imaging, discussion of fertility goals (if relevant), explanation of staging and molecular testing, and a clear plan for surgery and adjuvant therapy if needed. Many clinics also offer video consultations and second opinions for international patients.
FAQs
If I have post-menopausal bleeding, how urgent is evaluation?
Post-menopausal bleeding should be evaluated promptly — ultrasound and endometrial biopsy are standard first steps because early diagnosis improves curability.
Can molecular testing change my treatment plan?
Yes. Tests like MMR/MSI and POLE can identify patients who may benefit from immunotherapy or who have a better or worse prognosis, and these results increasingly drive therapy choices.
Is minimally invasive surgery as effective as open surgery for cure?
For appropriate patients, minimally invasive and robotic approaches provide equivalent oncologic outcomes with faster recovery and fewer complications; patient selection and surgeon experience matter.
What are my options if cancer returns after initial treatment?
Treatment depends on where and how the cancer recurs; options include surgery, radiation, chemotherapy, targeted therapy or immunotherapy, and participation in clinical trials at major centers.
How can I arrange a second opinion or fast workup in Spain?
Contact a gynecologic oncology specialist or a rapid-access clinic (many Spanish centers and private specialist practices, including clinics in Valencia, offer expedited assessments and teleconsultations). If you’d like, a specialist such as Dr. Minig can provide a second opinion and coordinate an accelerated diagnostic pathway.
Conclusion
So — is endometrial cancer curable? Often yes, particularly when it is diagnosed early and treated by a coordinated team that includes specialized surgeons, oncologists and pathologists. In Spain, strong specialist centers and evolving systemic therapies (including immunotherapy for selected molecular subtypes) provide real hope.If you or a loved one has been diagnosed, seeking a specialist gynecologic oncology opinion (for example with Dr. Lucas Minig or a local reference unit) is a practical first step toward the best possible outcome.