Don’t ignore abnormal bleeding. Learn how doctors distinguish cervical vs endometrial cancer—tests, treatments and when to see a specialist in Spain.
Introduction
This article answers a common question clearly: is cervical cancer the same as endometrial cancer? Below you’ll find a plain-language, clinically accurate breakdown of anatomy, causes, symptoms, screening, treatment for endometrial cancer and cervical cancer, and what to do if you live in Spain and need care. Read it like a friendly clinic conversation — short explanations, clear steps, and practical tips from a gynecologic oncology perspective.
Understanding the Female Reproductive Anatomy
Let’s locate the parts before we compare cancers.
What Is the Cervix?
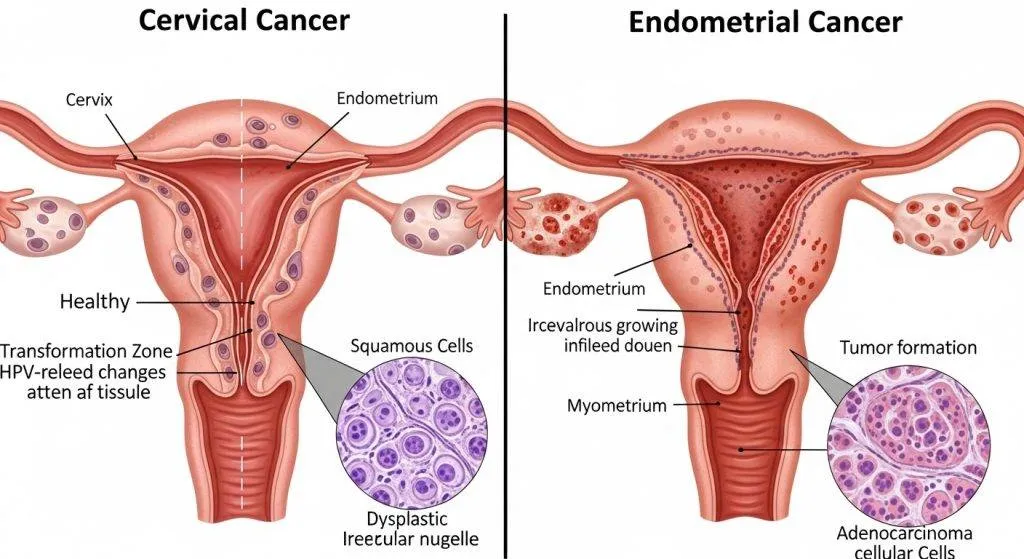
The cervix is the narrow, lower part of the uterus that opens into the vagina. Think of it as the house’s front door: small, exposed, and easy to inspect with screening tools like the Pap smear.
What Is the Endometrium?
The endometrium is the inner lining of the uterus — the soft tissue that thickens with hormones each month and is shed in a period. It’s more like the wallpaper of the room: it changes with cycles and responds strongly to hormones.
How Location Changes Everything?
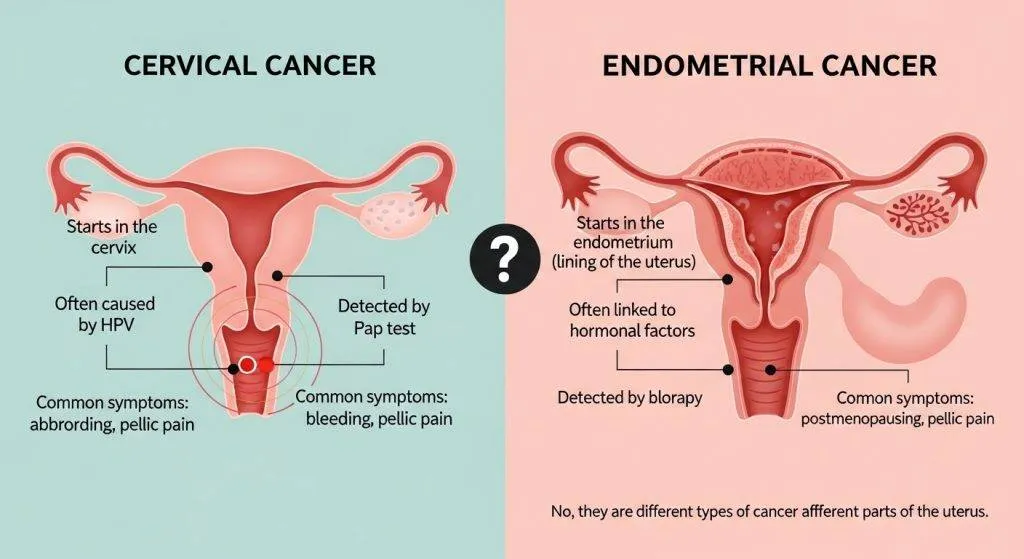
Where a tumor starts determines how it behaves, how we find it, and how we treat it. Cervical cancers begin at the “door” and are often HPV-driven; endometrial cancers start in the lining and are usually hormone- or metabolism-driven. That difference influences screening, symptoms, and therapy.
Is cervical cancer the same as endometrial cancer?
No. They are different diseases that happen in the same organ system but from different tissues, with different causes, screening methods and management. The rest of this guide explains exactly how and why they differ.
What is cervical cancer?
Cervical cancer arises from the cells that line the cervix. Because it’s a visible junction between vagina and uterus, the cervix is amenable to surface sampling (Pap) and HPV testing; early cell changes can be treated before invasive cancer develops. Cervical lesions often arise on the transformation zone — the exact place doctors inspect during a colposcopy.
Causes of cervical cancer
High-risk strains of HPV (for example, HPV-16 and HPV-18) are the dominant cause of cervical cancer. That is why primary prevention with HPV vaccination and secondary prevention through screening are so powerful. In many European programs the HPV test is replacing cytology as the primary screening tool because it detects risk earlier.
What is endometrial (uterine) cancer?
Endometrial cancer develops in the uterine lining (endometrium). The lining is internal and not routinely sampled unless symptoms occur. When the endometrium shows cancerous change, it’s usually because the tissue has been exposed to hormonal stimulation (for example, unopposed estrogen), or because of metabolic triggers. Detecting it usually requires an ultrasound or an endometrial biopsy.
Causes: Hormones, metabolism and endometrial cancer
Endometrial cancer risk rises with prolonged estrogen exposure without progesterone balance (e.g., certain HRT regimens, chronic anovulation), obesity, polycystic ovary syndrome, and insulin resistance. Research and European guidelines emphasize assessing metabolic health as part of risk reduction.
Who’s at risk? — comparing risk profiles
Ages, reproductive history, and lifestyle shape the two risk pictures differently.
Age & reproductive history
Cervical cancer commonly affects younger to middle-aged adults (though older women can also develop it); endometrial cancer peaks after menopause. Reproductive factors (like parity and age at menopause) modify endometrial risk; sexual history influences HPV exposure and thus cervical risk.
Lifestyle: obesity, smoking, sexual history
Obesity and metabolic disease are stronger drivers for endometrial cancer. Smoking increases the risk of some cervical cancers and can worsen outcomes. Sexual practices and number of partners influence HPV exposure and therefore cervical cancer risk.
Key differences at a glance
A quick snapshot that patients often want — read it like a checklist.
Cause
- Cervical: mainly high-risk HPV infection.
- Endometrial: hormonal imbalance, obesity, metabolic syndrome, some genetic syndromes.
Symptoms
- Cervical: post-coital bleeding, unusual discharge, later pelvic pain.
- Endometrial: abnormal uterine bleeding (especially post-menopause), heavier periods.
Screening Tests
- Cervical: organized screening with Pap smear and/or HPV testing.
- Endometrial: no routine population screening — investigated when symptoms arise with ultrasound/biopsy.
Typical Age Group
- Cervical: younger to mid-age adults.
- Endometrial: mostly postmenopausal women.
Symptoms: overlap and differences
Some symptoms overlap (bleeding, discharge), but how and when they appear helps clinicians decide which tests to run.
Abnormal bleeding: how to read the signs
Postmenopausal bleeding is a red flag for endometrial cancer and needs urgent assessment. Bleeding after intercourse or unusual post-coital bleeding suggests cervical pathology. Any new or persistent bleeding should prompt evaluation.
Other symptoms (discharge, pain, systemic signs)
Persistent malodorous discharge and pelvic discomfort may signal cervical disease or infection; systemic symptoms like weight loss or fatigue are usually later signs and warrant urgent work-up.
How is each cancer screened and diagnosed?
Screening catches cervical pre-cancer; endometrial cancer is usually diagnosed after symptoms.
Screening for cervical cancer (Pap smear, HPV)
Cervical screening programs use HPV testing and cytology to find precancerous lesions. HPV testing now often replaces cytology as primary screening in Europe because of higher protective value and longer intervals between tests. Colposcopy and targeted biopsies follow abnormal screens.
How is endometrial cancer usually found (ultrasound, biopsy)?
When bleeding occurs, the commonly used pathway is transvaginal ultrasound to measure endometrial thickness and an endometrial biopsy (an office procedure) to get tissue for histology. Hysteroscopy may be used if sampling is inconclusive. Guidelines and research projects in Europe are actively exploring better screening or triage tests for earlier detection.
When tests overlap and when they don’t
A Pap smear can occasionally detect some abnormal endometrial cells but is not reliable for endometrial cancer screening. Conversely, endometrial biopsy will not replace HPV testing for the cervix.
Treatment approaches: how they differ
Both cancers may require surgery, radiation, or systemic therapy — but the primary modalities and order differ.
Cervical cancer treatments
Early lesions: local excision (cone biopsy) or fertility-sparing procedures in selected patients. Larger or locally advanced disease often requires surgery and/or combined chemoradiation. Advanced diseases may need systemic therapy, including targeted agents or immunotherapy in specific settings.
Endometrial cancer treatments
Surgery is usually the first-line treatment (total hysterectomy ± removal of ovaries and staging). Adjuvant radiation or chemotherapy depends on risk features; low-grade, early disease may be treated surgically alone. Hormonal therapy is an option for very specific low-grade tumors when fertility preservation is desired.
Survival Rates and Prognosis – Does One Have a Better Outlook?
Prognosis depends mainly on stage; many endometrial cancers are caught early because of bleeding and have favorable 5-year survival, but high-risk subtypes exist.
European data and recent studies report relatively high 5-year survival for early-stage endometrial cancer (often >75–80% overall), while cervical cancer prognosis is excellent when detected early through screening programs. Nuanced survival comparisons depend on stage, tumor biology and treatments.
Symptoms that should make you see a doctor now
Don’t delay — bleeding is the key alarm bell.
- Any bleeding after menopause.
- Spotting or bleeding between periods.
- Bleeding after sex.
- Persistent pelvic pain or new abnormal discharge.
If you’re in doubt, call your GP or gynecologist. Quick evaluation (ultrasound, Pap/HPV test, or biopsy) is the right next step.
Prevention: vaccines, lifestyle, screening
Prevention is a combination of vaccination, screening, and healthy living.
- HPV vaccination prevents the majority of cervical cancers; Spain’s public programs recommend vaccination in childhood or adolescence and catch-up options are widely available.
- Cervical screening (Pap/HPV) finds precancerous changes early.
- Lifestyle measures (healthy weight, diabetes control) lower endometrial risk.
For patients in Spain — local pathways and what to expect
If you are in Spain, initial evaluation is typically via your primary care physician or gynecologist; public and private centers provide ultrasound and biopsy services. Spanish guidelines and regional oncology centers follow European recommendations for screening and management; second opinions and private consultations with gynecologic oncologists are commonly used to speed diagnosis and individualize treatment plans.
Meet Dr. Lucas Minig
Dr. Lucas Minig is a gynecologic oncologist with extensive experience in minimally invasive and complex pelvic surgery. In his practice he emphasizes rapid triage for bleeding, individualized staging, and offering fertility-sparing options when safe. Patients often tell Dr. Minig they value clear explanations: “two different cancers, two different pathways,” he says — and that clarity helps patients make confident decisions.
(Dr. Lucas Minig’s clinical approach blends guideline-based care with practical patient-centred counselling, particularly for patients traveling within Spain for a second opinion.)
Book a consultation: how to get a second opinion at care.drlucasminig.com
If you want a specialist review, many patients in Spain request a second opinion to confirm diagnoses or to consider minimally invasive surgical options. You can book an initial consult online or by contacting a clinic directly; bring imaging and pathology reports to speed the process. Dr. Lucas Minig and his team often provide telemedicine triage followed by targeted tests and an individualized treatment plan.
FAQs
Is a Pap smear enough to rule out endometrial cancer?
No — Pap smears screen the cervix for HPV-related changes. An endometrial biopsy or ultrasound is needed if uterine lining disease is suspected.
Can the HPV vaccine prevent endometrial cancer?
No — the HPV vaccine prevents HPV-driven diseases like cervical cancer; it does not prevent most endometrial cancers that are driven by hormones and metabolism.
I have postmenopausal spotting — what should I do?
Any postmenopausal bleeding should be evaluated promptly with a gynecologist, who will usually order a transvaginal ultrasound and consider an endometrial biopsy.
Can both cancers be treated without surgery?
Early cervical lesions may be treated with local excision; many endometrial cancers are primarily treated surgically. Non-surgical options exist in select cases (e.g., hormonal therapy for fertility preservation), but decisions depend on stage and tumor type.
How can I get a second opinion from Dr. Lucas Minig in Spain?
You can request a consultation at care.drlucasminig.com for telemedicine triage or in-person review; bring all reports and imaging so Dr. Lucas Minig can provide a focused plan quickly.
Conclusion
Cervical cancer and endometrial cancer are not the same. They differ in origin, causes, symptoms, screening, and typical treatments. HPV vaccination and organized cervical screening have transformed prevention of cervical cancer, while prompt attention to abnormal uterine bleeding remains the best route to early detection of endometrial cancer. If you have symptoms or abnormal screening results in Spain, seek evaluation promptly — and consider expert review from a gynecologic oncologist such as Dr. Lucas Minig if you want a focused second opinion.