Worried about atypical endometrial hyperplasia? Short, clear answer and next steps — Dr. Lucas Minig explains risks, treatments and fast video consults in Spain.
Introduction
Atypical endometrial hyperplasia (AEH) is a diagnosis that commonly raises alarm — and understandably so. The words “atypical” and “hyperplasia” sound serious, but they don’t mean the same thing as “invasive cancer.” In this long-form guide you’ll get a clear explanation of what AEH is, how doctors tell it apart from cancer, the real risks backed by data, practical treatment choices, how AEH is managed in Spain, and what to expect when you see a specialist. I’ll also explain Dr. Lucas Minig’s approach to AEH — practical, evidence-based, and patient-first — so you know how a specialist thinks about the tradeoffs between surgery and fertility-preserving care.
What Is Endometrial Hyperplasia?
Endometrial hyperplasia is simply an overgrowth of the cells that line the uterus (the endometrium). Under normal hormonal conditions the lining thickens and sheds in a predictable cycle; with hyperplasia, the glandular component becomes crowded and architectural patterns change. Hyperplasia is a spectrum — from innocuous (no atypia) to worrisome (with atypia). The presence or absence of atypia is the single most important histologic factor that guides treatment.
Simple Hyperplasia vs. Complex Hyperplasia
Pathologists often describe hyperplasia as:
- Simple hyperplasia: gland enlargement with little architectural complexity; usually low cancer risk.
- Complex hyperplasia: glands are crowded and irregular; higher concern than simple.
When atypia (cellular abnormalities) is present in either simple or complex hyperplasia, the term becomes more worrisome — and that’s when we call it atypical endometrial hyperplasia (AEH) or, in modern pathology, endometrial intraepithelial neoplasia (EIN).
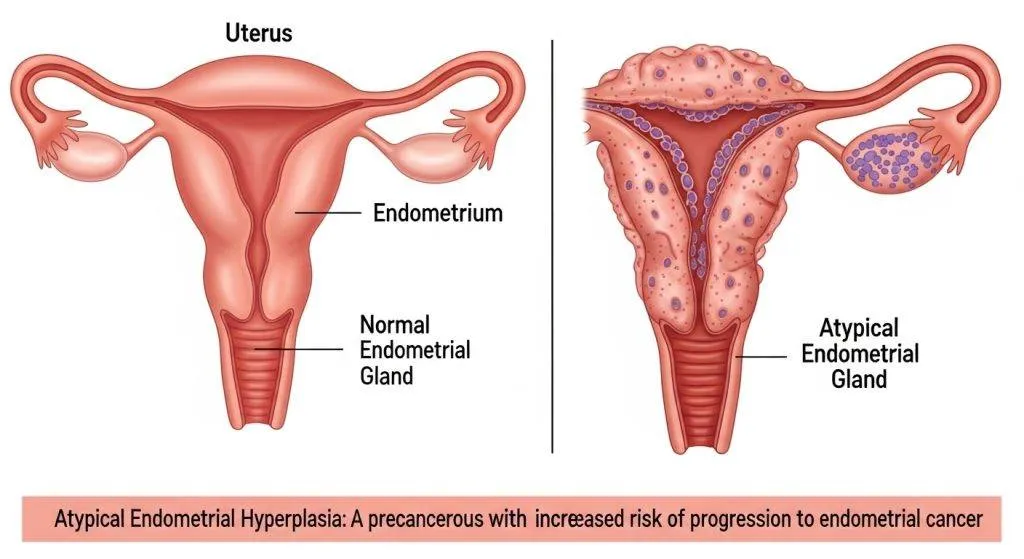
Normal uterine lining vs. hyperplasia
Think of the normal endometrium as a neatly planted lawn that grows and trims itself every month. Hyperplasia is like that lawn growing wildly, with patches of taller, irregular grasses (glands). The difference is obvious under the microscope but the clinical implications depend on whether the cells also look abnormal (atypia).
The role of hormones (estrogen and progesterone)
Endometrial hyperplasia is fundamentally a hormonal problem. Persistent unopposed estrogen stimulation — whether from obesity (peripheral aromatization), chronic anovulation (PCOS), estrogen therapy without progesterone, or certain medications like tamoxifen — drives glandular proliferation. Progesterone (or progestins) counteracts this effect and is the medical basis for conservative therapy.
Is Atypical Endometrial Hyperplasia Cancer?
No — AEH is not invasive cancer. The defining difference is invasion: cancer cells invade the myometrium (uterine muscle) or beyond; AEH is confined to the lining. However, AEH is clinically treated as a serious precancerous condition because of the substantial rates of coexisting or later carcinoma discovered in patients with AEH.
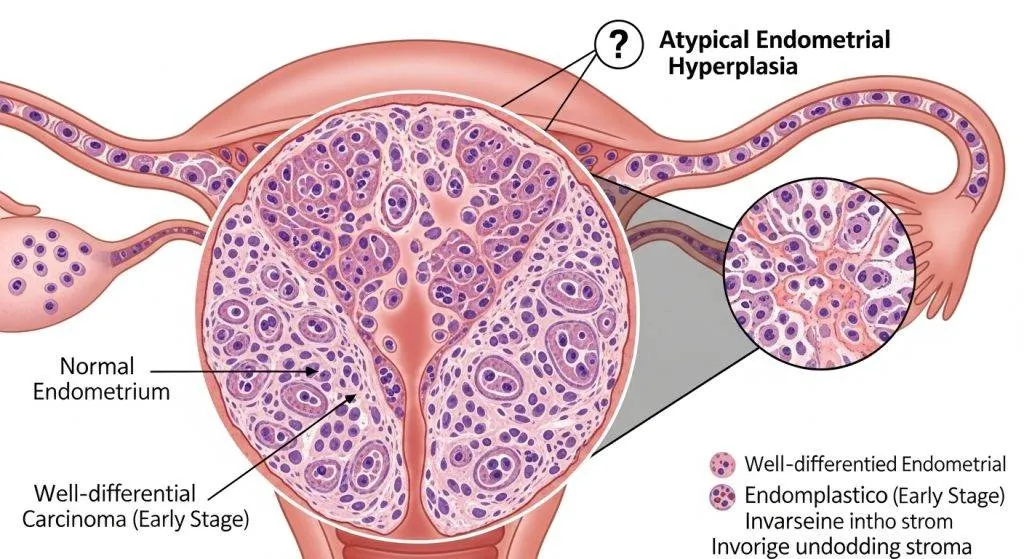
The Critical Difference — Invasion
- Precancerous (AEH/EIN): abnormal cells confined to the endometrium, no stromal or myometrial invasion.
- Invasive cancer: cells breach the basal layer and infiltrate the myometrium and potentially spread to lymph nodes or distant sites.
Why Doctors Call It a Precancerous Condition?
AEH has molecular and morphological abnormalities similar to early endometrioid carcinoma. Clinically, many patients with AEH will either have concurrent carcinoma found at hysterectomy or will progress to carcinoma over time — which is why clinicians often recommend definitive treatment or close monitoring.
How big is the risk? Statistics and realities
Understanding the numbers helps shape realistic expectations.
Risk of concurrent cancer at diagnosis
Studies vary by population and sampling methods; meta-analyses and recent series report a wide range. Some series found concurrent endometrial carcinoma in roughly 20–40% of women initially diagnosed with AEH on biopsy; smaller or single-centre reports have shown even higher proportions in selected cohorts. This variability is largely due to sampling differences and histopathologic interpretation.
Risk of progression if untreated
Longitudinal analyses estimate the progression risk to invasive cancer at roughly ~8% per year in some pooled data — cumulative progression increases over time, which supports proactive management decisions. Exact numbers depend on patient age, comorbidities, histologic assessments, and whether the AEH is treated.
How is AEH diagnosed? Tests and pitfalls?
Diagnosis rests on tissue sampling and histopathology; imaging and hysteroscopy are supportive.
Endometrial biopsy and hysteroscopy
- Transvaginal ultrasound (TVUS): good screening tool (measures endometrial thickness) but cannot diagnose AEH.
- Endometrial biopsy (pipelle): common office test — useful but may not sample focal lesions.
- Hysteroscopy with directed biopsy: provides visual inspection and targeted sampling; superior diagnostic accuracy and sensitivity compared with blind techniques. Whenever AEH is suspected, hysteroscopy increases the chance of finding focal carcinoma.
Why sampling can miss invasive cancer?
A sampling device can miss a small focus of carcinoma, especially if the malignancy is focal or located in an area not reached by the instrument. That’s why treatment decisions often consider both biopsy results and additional factors (imaging, patient risk profile), and why definitive hysterectomy specimens sometimes reveal occult carcinoma not seen on preoperative sampling.
Treatment options: a practical, patient-first approach
Management balances cancer risk, patient comorbidities, fertility desires, and informed choice.
Definitive surgery: hysterectomy (when recommended)
When childbearing is complete or the patient prefers definitive treatment, total hysterectomy (often with bilateral salpingo-oophorectomy in older patients) is recommended by many guidelines because it removes the lesion and any occult carcinoma and eliminates the risk of progression. Surgical planning is individualized; lymph node staging is not routinely performed for pure AEH but is considered if cancer is found on final pathology.
Fertility-sparing care: progestins and IUDs
Patients who want to preserve fertility may be offered medical therapy:
- High-dose oral progestins (medroxyprogesterone, megestrol) or
- Levonorgestrel-releasing IUD (LNG-IUS) — increasingly used because it delivers a high local progestin dose with fewer systemic effects.
Recent systematic reviews report high complete response rates for LNG-IUS at 12 months (many series >80%), though follow-up and patient selection matter. Conservative therapy requires rigorous surveillance and a clear plan to proceed to hysterectomy if there is no regression or if carcinoma emerges.
Surveillance protocol: what follow-up looks like
Typical conservative-management surveillance:
- Repeat endometrial sampling (biopsy) every 3 months until a complete response is documented.
- TVUS and clinical review between biopsies as needed.
- If persistent AEH or progression is documented, move to surgical management.
How AEH is managed in Spain?
Typical care pathways in private and public systems
In Spain, pathways vary by region and facility:
- Primary care/GP or gynecologist: initial evaluation for abnormal bleeding and TVUS.
- Public hospitals (SNS): referral to gynecology units for hysteroscopy and biopsy; multidisciplinary discussion for complex cases.
- Private clinics and specialty centers: often offer faster access to hysteroscopy, pathology second opinions, and combined fertility-oncology pathways. Telemedicine options (video consults) are widely available and commonly used for second opinions and preoperative counseling.
When to seek a specialist or second opinion?
Seek specialist input if:
- Your report shows atypical hyperplasia (AEH/EIN).
- You desire fertility preservation and wish to explore conservative options.
- Your biopsy is discordant with imaging or clinical concern persists.
A gynecologic oncologist or a specialized gynecology unit (esp. in larger Spanish cities) can offer expert assessment and tailored plans.
What to expect at a specialist consultation?
Questions your doctor will ask
- Age and fertility desires.
- Details of bleeding symptoms and duration.
- Medical history: obesity, diabetes, PCOS, hormone therapies, tamoxifen.
- Prior pathology and imaging results.
- Any prior fertility treatments or obstetric history.
Tests your doctor will order
- Review of the original pathology slide (or referral for pathology second opinion).
- Hysteroscopy with directed biopsy if not already performed.
- Pelvic imaging (TVUS, sometimes MRI) to assess for focal lesions or myometrial involvement.
- Blood tests to evaluate metabolic risks.
Meet Dr. Lucas Minig
Experience and approach to AEH and early endometrial disease
Dr. Lucas Minig is a gynecologic oncologist based in Valencia, Spain, with extensive experience in uterine pathology and minimally invasive techniques. His approach blends clear, evidence-based counseling with attention to patient values — whether the aim is fertility preservation or definitive cancer prevention. He emphasizes reviewing pathology directly, offering hysteroscopic assessment, and co-ordinating multidisciplinary care when needed.
What a video consult with Dr. Minig looks like?
A typical video consult includes a review of your history and pathology, discussion of management options (risks and timelines), and a personalized next step plan — whether that is immediate hysteroscopy, conservative progestin therapy with surveillance, or arranging definitive surgery in Spain. Remote patients across Spain use video consults to access specialist opinions before deciding on local care.
Practical tips: how to reduce your risk and prepare for treatment?
- Address modifiable risks: weight loss, glycemic control, and treatment of anovulation reduce estrogen excess.
- Screening for hereditary risk: if you have a strong family history of colorectal or endometrial cancer, ask about Lynch syndrome testing.
- Get complete documentation: obtain copies of pathology slides/reports and imaging before a second opinion.
- Plan for fertility: if you hope to conceive, discuss fertility preservation and timelines before definitive surgery.
Myth-busting: common misunderstandings
- Myth: AEH is the same as endometrial cancer.
Fact: AEH is premalignant, not invasive cancer — but it often coexists with cancer and requires treatment. - Myth: All AEH requires immediate hysterectomy.
Fact: Hysterectomy is the definitive treatment for most women who have completed childbearing, but carefully selected patients may pursue fertility-sparing progestin therapy under strict surveillance. - Myth: A single negative biopsy rules out cancer.
Fact: Sampling error is real; hysteroscopy and directed biopsy improve diagnostic accuracy and are often recommended before choosing conservative care.
FAQs
If my biopsy shows AEH, do I need a hysterectomy right away?
Not always. If childbearing is complete, hysterectomy is often recommended because it removes both lesion and uncertainty. If fertility preservation is desired, conservative therapy with close surveillance is an option in selected patients — but this requires careful diagnostic confirmation that invasion is not present.
How effective is the levonorgestrel IUD for AEH?
The levonorgestrel-releasing IUD (LNG-IUS) achieves high local progestin levels and shows substantial regression rates in many studies; it is a widely used fertility-sparing option when criteria are met.
Can AEH come back after treatment?
After hysterectomy recurrence in the uterus is not possible, but if conservative treatment is used there is risk of persistence or recurrence and ongoing surveillance is essential.
Should I get a second pathology review?
Yes — obtaining review by a gynecologic pathologist is recommended when AEH is diagnosed, especially if conservative management is being considered. Variability in pathology interpretation affects management.
How urgent is evaluation for postmenopausal bleeding?
Postmenopausal bleeding is always an indication for prompt evaluation because it may be the first sign of AEH or endometrial cancer. Don’t delay — ask for expedited sampling and a specialist referral when appropriate.
Conclusion
Atypical endometrial hyperplasia is not the same as invasive cancer, but it is a serious precancerous condition that deserves rapid, evidence-based evaluation. Options range from definitive hysterectomy — commonly recommended when fertility is complete — to fertility-sparing strategies using progestins or an LNG-IUS under tight surveillance. In Spain, you can access multidisciplinary care in both public and private settings; specialists such as Dr. Lucas Minig combine surgical expertise with conservative options and offer video consultations for patients across the country. If you’ve been diagnosed with AEH, prioritize a specialist review, gather your biopsy reports, and ask about both immediate treatment and a clear follow-up plan.