Quick guide to how long endometrial cancer take to develop, modifiable risks, and when to seek care — includes insights from Dr. Lucas Minig.
Introduction
Endometrial cancer develops in the lining of the uterus and — depending on biology and risk factors — can take years to form or, in some cases, progress much faster. This piece walks through the usual timeline, the biological steps, and the things that speed up or slow down development, with practical notes for patients in Spain and how clinicians like Dr. Lucas Minig typically approach the question of “how long.”
How Long Does Endometrial Cancer Take to Develop?
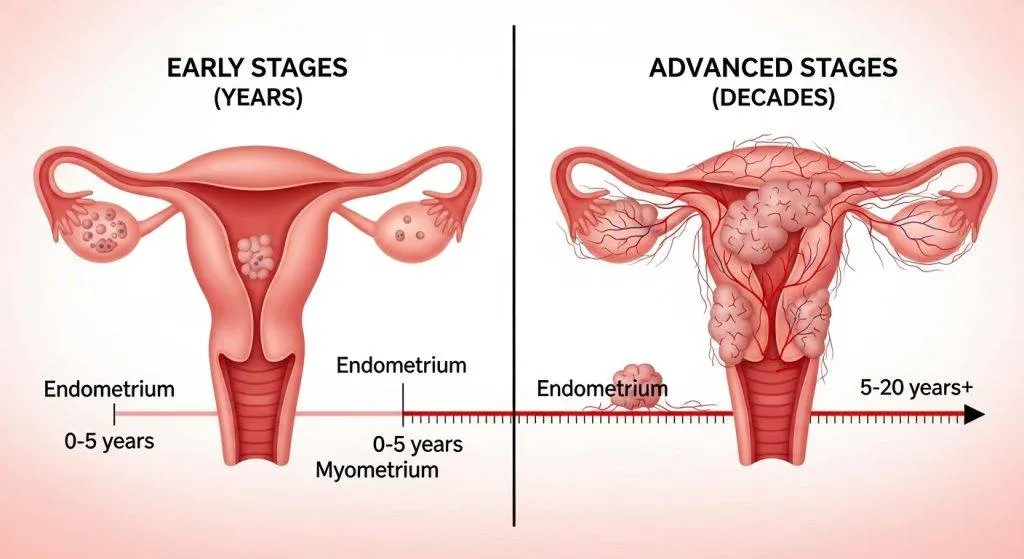
Most commonly, the process is gradual and measured in years rather than months.
The Slow-Growing Nature of Most Cases
For the common, estrogen-driven (Type 1) cancers, development usually follows a predictable path: normal lining → hyperplasia → atypia → carcinoma. This often takes several years (commonly 5–10 years), giving clinicians time to detect precancerous changes and intervene.
When Development Can Be Faster
Not all cases follow that slow arc. Aggressive subtypes (for example, serous or clear cell types) can appear and progress more quickly — sometimes within 1–3 years — and may be less obviously linked to long-standing hormonal imbalances.
Why “how long” vary so much?
Timescales differ because cancer is not a single process — it’s many processes influenced by biology and environment.
Biological factors (grade, subtype, genetics)
Tumor grade and subtype matter. Low-grade endometrioid tumors generally accumulate mutations slowly. High-grade tumors (and certain molecular profiles) divide quickly and metastasize earlier. Inherited mutations — notably Lynch syndrome — can also shorten the timeline to cancer.
Modifiable risk factors (obesity, hormones, diabetes)
Lifestyle and medical exposures shape the pace of change. Obesity increases estrogen activity, diabetes/insulin resistance create a pro-growth metabolic state, and certain hormone therapies (like estrogen without progesterone) remove the checks that normally keep the endometrium from overgrowing.
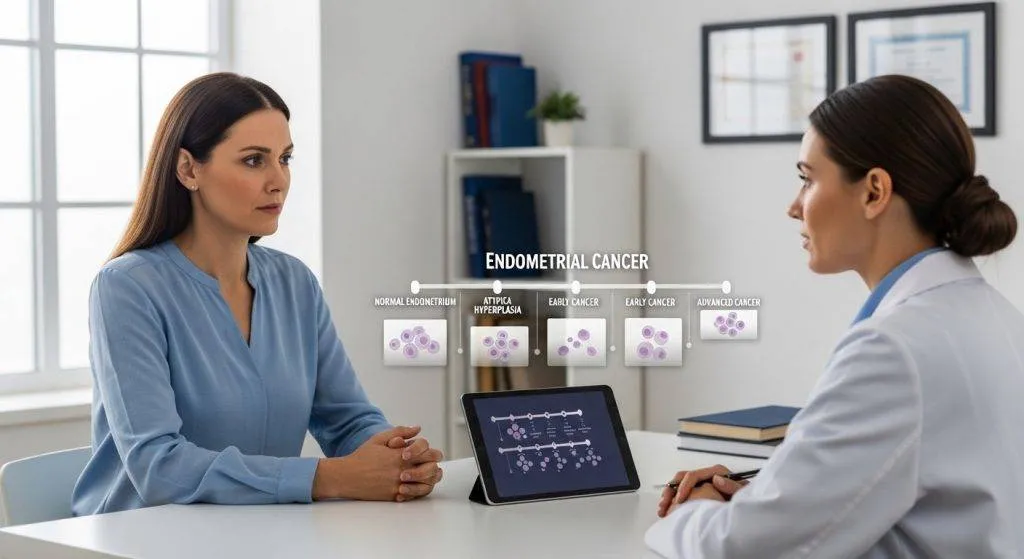
The Step-by-Step Development of Endometrial Cancer
Below is the usual biological sequence. Each step is a chance to detect and halt progression.
Step 1 – Hormonal imbalance (Unopposed estrogen)
Unopposed estrogen — whether from body fat, ovarian dysfunction, or external therapy — stimulates the endometrium continuously. Without progesterone’s balancing effect, the lining thickens and cells replicate more than they should.
Step 2 – Endometrial hyperplasia
Hyperplasia is an overgrowth of the endometrium. It’s a warning sign — not cancer yet — and is categorised by whether cells look abnormal.
- Hyperplasia without atypia: This form often behaves benignly. Many cases regress with treatment (for example, with progesterone therapy) or with removal of the estrogen stimulus. Progression to cancer is relatively uncommon but not impossible.
- Atypical hyperplasia (EIN): Atypical hyperplasia — also called endometrial intraepithelial neoplasia (EIN) — carries a much higher risk of progressing to invasive cancer. Because of that risk, doctors in Spain and elsewhere usually recommend closer monitoring, progestin therapy when fertility preservation is desired, or definitive surgery once childbearing is complete.
Step 3 – Early-stage carcinoma
When cells invade beyond the surface lining into the myometrium or form a tumor mass, the condition is cancer. Most early-stage cases are still highly treatable, particularly because bleeding often prompts earlier testing.
Step 4 – Advanced progression (if untreated)
If left unchecked, cancer can invade deeply into the uterus, spread to lymph nodes, and metastasize. The speed of this progression depends on tumor biology: Type 1 often remains local longer; Type 2 can become advanced more rapidly.
Slow-Growing vs Aggressive Types
Different histologies behave differently — that’s why timelines vary.
Type 1 (Endometrioid adenocarcinoma)
This is the most common form. It’s usually estrogen-driven, low to intermediate grade, and slow-growing. Many patients present early because of abnormal uterine bleeding — a symptom that triggers evaluation and biopsy.
Type 2 (Serous and clear cell carcinoma)
These are less common but more aggressive. They aren’t typically linked to estrogen excess and can present at more advanced stages. Because they may not follow the “hyperplasia-first” model, they can seem to arise quickly.
What Factors Influence How Fast It Develops?
Some factors are within our control; others are not.
Obesity and metabolic syndrome
Excess adipose tissue converts androgens to estrogens, increasing unopposed estrogen exposure. Obesity also correlates with inflammation and insulin resistance — both of which can promote tumor growth.
PCOS and irregular ovulation
Chronic anovulation means long stretches without progesterone’s stabilizing influence. That increases the risk of hyperplasia and speeds the path to malignant transformation.
Estrogen-only hormone therapy
When estrogen is given without a progestin (in women with a uterus), the risk of endometrial overgrowth rises. In Spain and other countries, clinicians carefully balance menopausal symptom relief against that risk.
Genetics and Lynch syndrome
Inherited predispositions (notably Lynch syndrome) sharply raise lifetime risk and often cause earlier onset. If there’s a family history of colorectal or uterine cancer, genetic counseling is recommended.
Age and Menopause
Most diagnoses occur after menopause — commonly between ages 55–65 — which reflects the long cumulative effect of exposures. That said, younger women with risk factors can still develop disease.
Early Symptoms That Appear During Development
Symptoms tend to show up before late-stage spread — that’s a critical advantage.
Abnormal Uterine Bleeding
In premenopausal women, heavier or irregular bleeding that’s a departure from the usual pattern is the most common early sign.
Postmenopausal Bleeding
Any vaginal bleeding after menopause is alarming and should prompt urgent evaluation. Many cases of endometrial cancer are found this way.
Pelvic Pain and Advanced Signs
Pelvic pain, weight loss, or systemic symptoms generally appear later, often with more advanced disease.
How Is It Diagnosed in Spain?
Spain has public and private services that perform the typical diagnostic pathway — ultrasound, biopsy, and specialist assessment.
Ultrasound and Endometrial Thickness
Transvaginal ultrasound is a first-line test to measure endometrial thickness. A thickened lining in a postmenopausal woman often prompts biopsy.
Endometrial Biopsy
An office biopsy is the standard way to sample the lining. It’s quick and usually diagnostic.
Hysteroscopy and Imaging
If a biopsy is inconclusive, hysteroscopy lets a clinician directly view and sample suspicious areas. MRI is used to assess depth of invasion and aid staging when cancer is diagnosed.
The Role of Gynecologic Oncologists
Specialist surgeons (gynecologic oncologists) guide treatment decisions — from minimally invasive surgery to when adjuvant therapy is needed. In clinic practice, experienced doctors such as Dr. Lucas Minig work with multidisciplinary teams to tailor the timing and extent of intervention depending on tumor biology and patient goals.
Can Endometrial Cancer Be Prevented?
While not all cancers are preventable, risk can often be reduced.
Hormonal Balance and Progesterone
Using combined hormonal therapy (estrogen + progestin) when needed, or progestin-releasing intrauterine systems in high-risk patients, can reduce endometrial proliferation.
Weight Management
Losing weight and improving metabolic health decrease estrogen production by adipose tissue and lower risk.
Regular Gynecologic Check-Ups
Surveillance for women with risk factors — particularly those with Lynch syndrome or long-standing anovulation — catches hyperplasia or early cancer when it’s easiest to treat.
Can It Develop Quickly in Young Women?
Yes — albeit less commonly. Young women with PCOS, obesity, or genetic predisposition can develop atypical hyperplasia or even carcinoma sooner than expected, so abnormal bleeding at any age deserves evaluation.
Why Early Detection Changes Everything?
Because most endometrial cancer starts in the lining and often causes bleeding, it’s frequently detected at an early, highly treatable stage. Early diagnosis widens options — from fertility-sparing medical therapy to minimally invasive surgery — and improves survival.
How a specialist (e.g., Dr. Lucas Minig) approaches patients worried about timing
A specialist will personalize both the diagnostic timeline and the management plan. In practice this means:
- Rapid assessment of symptoms and risk factors (history, BMI, family history).
- Timely imaging and office biopsy to resolve uncertainty.
- Multidisciplinary discussion where needed (pathology review, imaging staging).
- Clear communication about expected timelines, options (surveillance vs treatment), and implications for fertility and menopause.
Dr. Lucas Minig’s approach in Spain focuses on minimizing delay, offering minimally invasive options where appropriate, and giving patients practical guidance on modifying risk factors while planning definitive care.
FAQs
Can endometrial cancer develop in less than a year?
It’s uncommon for typical Type 1 cancers, but aggressive subtypes or specific circumstances can lead to faster development. Any new abnormal bleeding deserves prompt assessment.
If I have atypical hyperplasia, how urgent is treatment?
Atypical hyperplasia carries a higher progression risk. Your doctor may recommend close follow-up, medical management, or surgery depending on age, fertility plans, and other factors.
Does losing weight really make a difference?
Yes — weight loss reduces estrogen produced by fat tissue and lowers inflammation and insulin resistance, all of which reduce endometrial stimulation and long-term risk.
What should I do if I notice postmenopausal bleeding in Spain?
See your primary care doctor or gynecologist immediately. Clinics in Spain commonly perform ultrasound and biopsy quickly; a referral to a gynecologic oncologist is arranged if needed.
Who should I consult for a second opinion?
Seek a gynecologic oncologist or a multidisciplinary cancer center. Specialists like Dr. Lucas Minig are experienced in explaining timelines, risks, and tailored treatment options.
Conclusion
“How long does endometrial cancer take to develop?” is not a one-size-fits-all question. For many people the process is gradual and measured in years, often beginning with reversible hyperplasia; for others — particularly with aggressive subtypes or genetic predisposition — the course may be more rapid. The best defense is awareness: report abnormal bleeding immediately, address modifiable risks (weight, metabolic health), and seek specialist assessment when needed. In Spain, you’ll find coordinated care pathways and experienced gynecologic oncologists who can clarify timelines and recommend an individualized plan.