Fluid in the endometrial cavity doesn’t always mean cancer. Read a clear, evidence-based guide from Dr. Lucas Minig (Valencia, Spain) — know when to worry and what tests to ask for
Introduction
Hearing that an ultrasound shows fluid in the endometrial cavity can be unsettling. Many women immediately jump to the worst-case scenario: Does fluid in the endometrial cavity mean cancer? It’s a completely understandable fear. After all, the uterus isn’t supposed to be “filled” with anything, right?
This guide walks you step-by-step through what endometrial cavity fluid (EFC) means, when clinicians become concerned, how doctors in Spain (including Dr. Lucas Minig in Valencia) evaluate it, and what the typical diagnostic and treatment pathways look like.
What is endometrial cavity fluid (EFC)?
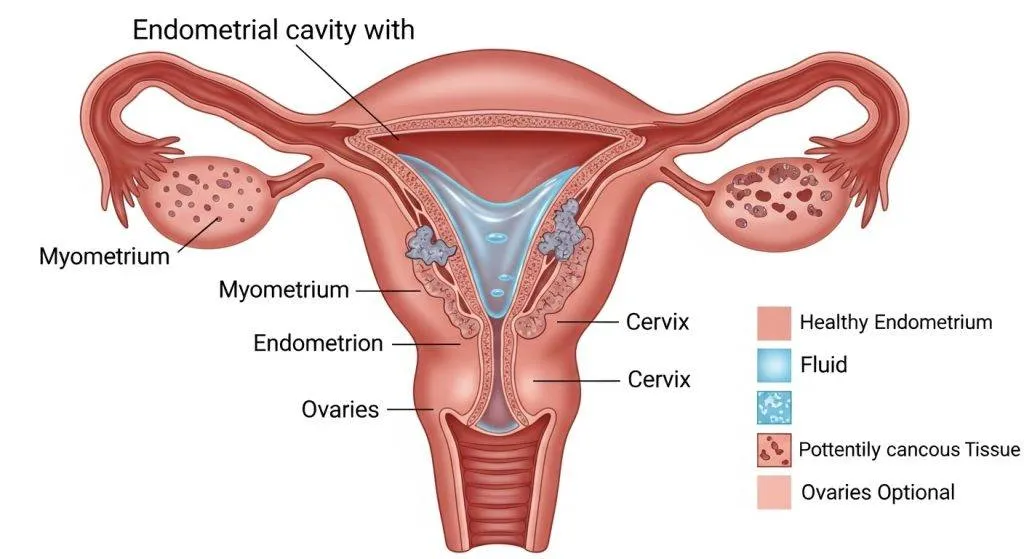
Endometrial cavity fluid refers to liquid seen inside the uterine cavity on imaging, usually during a transvaginal ultrasound. The uterine cavity is normally a potential space — its walls touch. When fluid appears, it separates those walls, making it visible on the scan.
Types of fluid seen on ultrasound
Ultrasound can broadly characterize fluid as:
- Anechoic (simple/clear) fluid — appears black on ultrasound and usually indicates serous or clear fluid.
- Echogenic (complex) fluid — contains internal echoes or debris and suggests blood, pus, necrotic tissue, or cellular material.
- Layered or particulate fluid — may indicate sludge, blood clots, or septations and often prompts further evaluation.
How radiologists describe fluid (simple vs echogenic)
Radiology reports typically flag whether fluid is anechoic (simple) or echogenic/complex. This descriptor guides urgency: echogenic fluid frequently triggers additional investigation because it correlates more often with intracavitary pathology (including malignancy), while simple anechoic fluid in an otherwise low-risk patient may prompt conservative follow-up.
Does Fluid in the Endometrial Cavity Mean Cancer?
No — not by itself.
Fluid alone is not a diagnosis. It’s a sign, not a disease.
However, in particular clinical settings (especially postmenopausal women with echogenic fluid or associated endometrial thickening) the probability of malignancy rises and merits prompt investigation.
Multiple large series show that while malignancy can be present, the absolute risk depends heavily on menopausal status, symptoms (for example post-menopausal bleeding), endometrial thickness and the ultrasound appearance of the fluid.
Common benign causes of fluid in the uterine cavity
There are several benign reasons why a uterine cavity fills with fluid. The clinical history and ultrasound appearance usually help clinicians sort these out.
Physiologic menstrual or ovulatory fluid
In premenopausal women, small amounts of fluid may be normal around ovulation or during menstruation—resulting from cyclical secretions or transient collection after shedding. This is often a benign, self-limiting finding.
Cervical stenosis and hydrometra
If the cervical canal is narrowed or obstructed (from prior procedures, scarring, or atrophy), normal uterine secretions or transudate can’t drain, producing a hydrometra (fluid-filled uterus). Cervical stenosis is more common after instrumentation, in older women or after radiation.
Benign intracavitary lesions (polyps, submucous fibroids)
Endometrial polyps and submucous fibroids can trap fluid and disrupt drainage, causing a visible collection. These lesions often produce focal echoes, filling defects on saline infusion sonography, or distend the cavity — and are frequently treatable with office hysteroscopy or polypectomy.
Infection and pyometra
Infective collections (purulent fluid, or pyometra) create echogenic, often complex fluid and are accompanied by systemic or local symptoms (fever, pain, foul discharge). Pyometra in older or immunosuppressed patients requires expedient drainage and antibiotic therapy and sometimes image-guided interventions.
When should clinicians worry about cancer?
Not all fluid is dangerous, but clinicians become concerned when several specific risk factors or sonographic red flags are present.
The role of age and menopausal status
Postmenopausal women with endometrial fluid are at higher risk for underlying malignancy than premenopausal women. Asymptomatic premenopausal EFC is usually of low concern, whereas EFC in a postmenopausal patient, especially with additional risk factors, triggers a more aggressive diagnostic pathway.
Symptoms that increase concern (post-menopausal bleeding, persistent pain)
Red-flag symptoms include:
- Postmenopausal bleeding
- Unexplained vaginal bleeding
- Persistent pelvic pain
- Unintentional weight loss (less common)
Bleeding plus fluid is much more suspicious than fluid alone.
Ultrasound red flags: echogenic fluid, debris, and thickened endometrium
Echogenic/complex fluid, mobile debris, or an accompanying thickened endometrial stripe on transvaginal ultrasound are imaging features associated with higher rates of malignancy or significant pathology. Endometrial thickness thresholds in symptomatic women have been validated: for example, an endometrium >5 mm in a bleeding postmenopausal woman carries substantially greater risk; thicker measurements (eg. >11 mm) further increase that risk.
Evidence: what the studies say about malignancy risk?
Large observational series and meta-analyses provide practical estimates of how often EFC corresponds to cancer, and how that varies by context.
Postmenopausal fluid and the estimated risk (summary of key studies)
Several studies report that postmenopausal women with endometrial fluid have a low but clinically relevant malignancy rate—one pooled analysis and single-center studies put the malignancy rate around 1–3% overall, with higher rates when fluid is echogenic or accompanied by endometrial thickening or bleeding. Given the population prevalence, many experts recommend endometrial sampling in symptomatic postmenopausal women with EFC.
How frequently fluid alone represents cancer
Isolated simple fluid in an asymptomatic postmenopausal woman carries a low absolute risk; however, fluid that is echogenic, associated with focal masses, or occurs alongside endometrial thickening is more often linked to malignancy. The precise frequency varies by cohort, but clinicians treat the combination of risk factors (age + bleeding + complex fluid + thickened endometrium) as especially concerning.

Diagnostic pathway: what doctors do next (step-by-step)
When endometrial fluid is identified, clinicians follow a practical and evidence-based sequence to reach a diagnosis while minimizing unnecessary invasive tests.
Transvaginal ultrasound (TVUS) — first line
TVUS is the first-line imaging test: it documents the presence, volume and sonographic character of the fluid, measures endometrial thickness, and looks for focal masses. In postmenopausal bleeding, TVUS helps stratify risk and decide whether sampling is needed. However, TVUS is not a perfect screen and cannot always visualize intracavity lesions clearly.
Saline infusion sonography (SIS) and diagnostic hysteroscopy
If TVUS is inconclusive or shows intracavitary suspicion (polyps, filling defects or complex fluid), saline infusion sonography (SIS) —also called sonohysterography—improves cavity delineation and helps detect focal lesions without immediate surgery. Diagnostic hysteroscopy (with direct visualization) is the gold standard for identifying and treating focal pathology when needed. SIS and hysteroscopy are complementary tools used depending on local resources and patient factors.
Targeted endometrial biopsy and histology
When imaging or symptoms raise concern, clinicians obtain an endometrial sample (office endometrial biopsy or hysteroscopy-guided biopsy) to establish histologic diagnosis. Biopsy confirms or excludes hyperplasia and carcinoma—decisions about management (conservative therapy vs surgery) depend on histology, imaging and patient aims (fertility preservation vs definitive treatment).
Treatment options depending on cause
Management is cause-specific and ranges from conservative medical therapy to definitive surgery and multidisciplinary oncologic care.
Treating benign causes (polypectomy, antibiotics, cervix dilation)
- Polyps/submucous fibroids: removed via hysteroscopic polypectomy or myomectomy.
- Cervical stenosis/hydrometra: managed by dilation or addressing the obstructing lesion.
- Infection/pyometra: urgent drainage and targeted antibiotics are required, with image-guided drainage if needed. These interventions often resolve fluid collections and symptoms.
Treating malignancy (surgical and multidisciplinary options)
When biopsy confirms malignancy, standard care usually involves surgical staging (hysterectomy ± bilateral salpingo-oophorectomy) tailored to histologic type and stage, often supported by a multidisciplinary team (gynecologic oncology, medical oncology, radiation oncology). In selected early cases and for fertility preservation, conservative hormonal approaches can be considered under strict surveillance. Multidisciplinary centers like Dr. Lucas Minig’s clinic in Valencia coordinate individualized treatment plans that integrate minimally invasive surgery and oncologic follow-up.
Practical advice for patients in Spain (local context)
If you live in Spain and your ultrasound report mentions endometrial fluid, the local healthcare pathway is accessible and often rapid.
How Spanish clinics (and doctors like Dr. Lucas Minig in Valencia) approach EFC
Spanish gynecology services typically begin with TVUS and clinical assessment; if red flags exist, many clinics offer expedited SIS, office hysteroscopy and biopsy. Specialists (including gynecologic oncologists such as Dr. Lucas) emphasize timely evaluation for postmenopausal bleeding or echogenic fluid and provide options for same-day or fast-track consultations depending on urgency.
When to seek urgent review and what to bring to your appointment
Seek prompt review for postmenopausal bleeding, fever with pelvic pain, or worsening discharge. Bring prior imaging, the ultrasound report (including screenshots if available), a list of medications, menstrual history and any prior gynecologic procedures—this helps the clinician triage and plan the correct next test without delay.
Why choose Dr. Lucas Minig in Spain?
Many patients prefer care that combines surgical expertise, rapid diagnostics and a clear pathway for both local and international patients.
Experience and expertise: what sets Dr. Lucas apart
Dr. Lucas Minig provides specialized gynecologic oncology experience with a focus on minimally invasive surgery, fertility-sparing options when appropriate, and integrated decision-making for endometrial pathology.
Patient pathway at Dr. Lucas’s clinic: tests, timing, and care
The clinic offers coordinated TVUS review, expedited SIS and hysteroscopy scheduling, targeted biopsy and tailored management plans—minimizing waiting times and uncertainty for patients.
International and local patients: video consults and fast scheduling
For non-local patients or those preferring remote consultations, the clinic arranges secure video consultations, remote review of imaging reports, and streamlined scheduling for in-person procedures when required.
FAQs
Is endometrial fluid usually dangerous?
Generally no—especially in premenopausal women. However, in postmenopausal women or when the fluid is echogenic or associated with a thickened endometrium, further testing is warranted.
What tests will my doctor order after finding fluid?
Most clinicians start with a transvaginal ultrasound; if results are suspicious, they proceed to saline infusion sonography, hysteroscopy and targeted endometrial biopsy.
Can infection cause EFC and how is it treated?
Yes—pyometra or endometritis can cause echogenic, often symptomatic fluid and is treated with drainage and antibiotics; severe cases may need image-guided or surgical intervention.
If I’m postmenopausal and have fluid but no bleeding, do I still need a biopsy?
Many specialists recommend evaluation (imaging + possible biopsy) for postmenopausal EFC because the risk of malignancy, while low, is clinically meaningful—especially with additional sonographic risk features.
How quickly can I see a specialist in Spain like Dr. Lucas Minig?
Availability varies, but many Spanish clinics offer expedited appointments or video consultations concerning findings; bring your ultrasound report and prior records to speed up assessment and planning.
Conclusion
Endometrial cavity fluid is a common ultrasound finding with a wide differential diagnosis. Most occurrences are benign—especially in premenopausal women—but certain features (postmenopausal status, echogenic or complex fluid, endometrial thickening, or bleeding) necessitate timely evaluation with TVUS, SIS and targeted biopsy. Evidence-based pathways reduce unnecessary invasiveness while ensuring malignancies are detected early. In Spain, centers and specialists such as Dr. Lucas Minig provide rapid, evidence-based assessment and management, balancing conservative options with definitive care when needed. If you have symptoms or a concerning ultrasound report, consult a gynecologist promptly—bring your reports and ask about targeted diagnostic steps like SIS and hysteroscopy.