Evidence-based answers on PCOS and uterine cancer risk, when to test, and fertility-preserving options — expert care from Dr. Minig in Valencia, Spain.
Introduction
Polycystic Ovary Syndrome (PCOS) is one of the most common endocrine disorders affecting reproductive-age women worldwide. A frequent and important clinical question is: can PCOS cause endometrial cancer? The relationship matters because PCOS often produces chronic hormonal patterns that increase stress on the uterine lining over years. This section summarizes why that connection exists, what it looks like clinically, and what practical steps patients and clinicians take to reduce risk — particularly in the context of specialist care available in Spain (for example, services offered by Dr. Lucas Minig and other gynecologic oncologists).
What Is PCOS (Polycystic Ovary Syndrome)?
PCOS is a heterogeneous syndrome defined by a combination of signs and symptoms that reflect ovarian dysfunction and metabolic disturbance. The core features typically include irregular menstrual cycles (oligo- or amenorrhea), clinical or biochemical hyperandrogenism (acne, hirsutism), and polycystic ovarian morphology on ultrasound — though not all patients have every feature. The syndrome reflects altered interactions among the hypothalamus, pituitary, ovary, adipose tissue and insulin pathways.
In practice, PCOS is best understood as a chronic condition that alters normal cyclical ovarian function and, importantly for this discussion, frequently prevents regular ovulation.
Common symptoms women experience
- Irregular or absent periods (the most common presenting complaint)
- Excess hair growth (hirsutism), acne, and sometimes male-pattern hair thinning
- Weight gain or difficulty losing weight; many patients show central adiposity
- Infertility or difficulty conceiving due to anovulation
- Fatigue and mood symptoms related to metabolic and hormonal changes
Symptoms vary widely; some patients have mild signs while others present with significant metabolic disease.
Can PCOS Cause Endometrial Cancer?
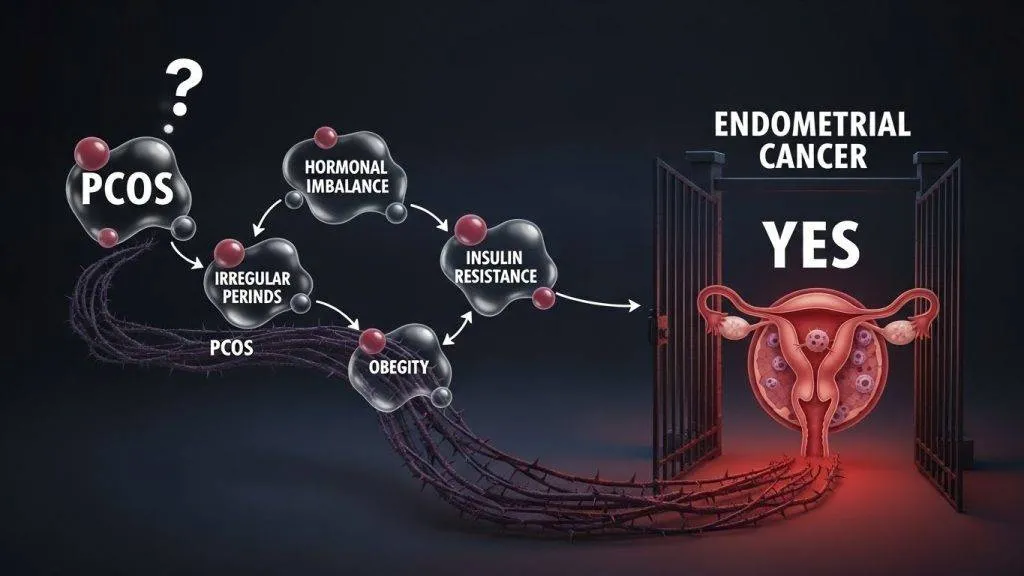
Strictly speaking, PCOS is not a direct carcinogen — it does not cause cancer by producing a specific mutational event. Rather, PCOS creates a hormonal and metabolic milieu that increases the likelihood that endometrial cells will undergo abnormal proliferation and, over time in some patients, malignant transformation. In plain language: PCOS raises the risk of endometrial hyperplasia and, in some cases, endometrial cancer — but it does not inevitably cause cancer in every patient.
Increased risk explained simply
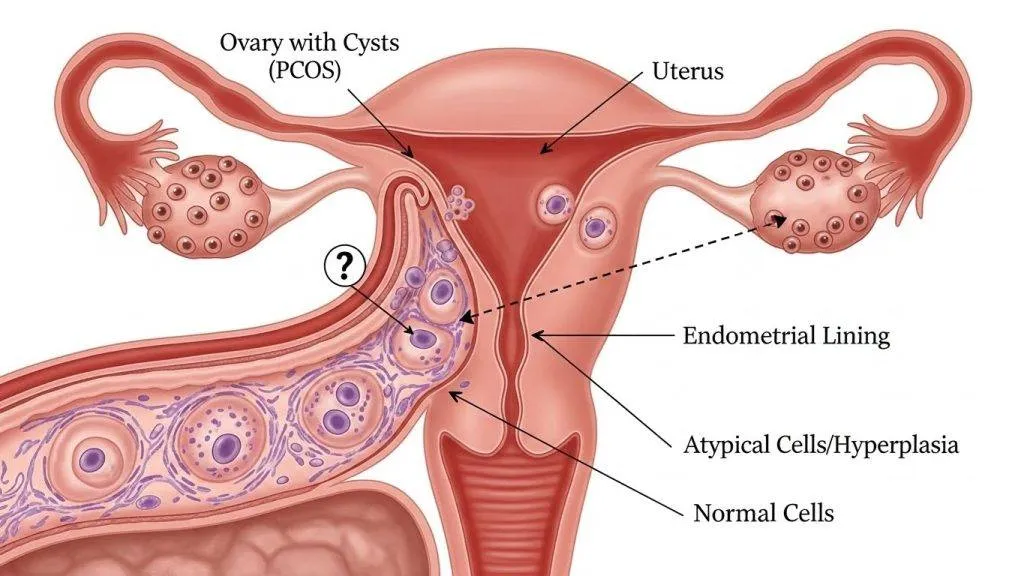
Because PCOS often produces repeated or sustained growth signals to the endometrium (largely via unopposed estrogen), the uterine lining can become persistently thickened (hyperplasia). Over years, and especially when combined with other risk factors such as obesity and insulin resistance, hyperplasia can progress to atypia and then to carcinoma in a minority of cases. Thus, the clinical emphasis is on recognition, surveillance and management to intercept disease at a reversible stage.
The Hormonal Link Between PCOS and Endometrial Cancer
The hormonal interaction is the core mechanism connecting PCOS and uterine lining changes: persistent estrogenic stimulation with inadequate progesterone protection.
Unopposed estrogen — the core problem
- Estrogen drives endometrial proliferation.
- Progesterone counterbalances that effect by stabilizing and shedding the lining during a normal cycle.
- In PCOS, lack of regular ovulation means little or no progesterone exposure — leaving the endometrium exposed to “unopposed estrogen.”
Lack of progesterone and irregular ovulation
- Ovulation releases the corpus luteum, which produces progesterone.
- Without ovulation (anovulation), that luteal phase never occurs, and progesterone pulses are absent or insufficient.
Why missed periods are not “harmless”
- Missing periods may feel convenient, but chronically absent shedding allows the lining to thicken quietly.
- Over years, that persistent thickening may result in atypical cells (hyperplasia) and, eventually, malignancy in a subset of cases.
How High Is the Risk for Women With PCOS?
Risk assessment must distinguish between relative risk (compared to people without PCOS) and absolute risk (overall chance over a lifetime).
Relative risk vs absolute risk
Epidemiologic studies show that women with PCOS have a higher relative risk of endometrial hyperplasia and endometrial cancer compared to women without PCOS — estimates vary, but many analyses report a 2–4× increased relative risk. It is important to interpret this in context: the absolute lifetime risk of endometrial cancer remains relatively low for most individuals, but it is meaningfully higher in the presence of sustained risk factors.
Does age increase the danger?
Yes. Risk increases with cumulative years of unopposed estrogen exposure and with age, particularly as the protective effect of regular cycles is absent over time. In addition, postmenopausal bleeding in a woman with a history of PCOS should be evaluated promptly because the baseline likelihood of endometrial pathology becomes proportionally more important with advancing age.
Additional Risk Factors That Make PCOS More Dangerous
PCOS often coexists with other conditions that further raise endometrial risk; addressing them reduces overall danger.
Diabetes and metabolic syndrome
Metabolic syndrome and type 2 diabetes increase inflammation and hormonal dysregulation — compounding the risk created by PCOS.
Obesity and insulin resistance
- Excess adipose tissue increases peripheral estrogen production via aromatization.
- Insulin resistance drives higher insulin and IGF levels, which can promote endometrial proliferation.
Family history of gynecologic cancers
- A family history of endometrial or colorectal cancers may indicate hereditary syndromes (e.g., Lynch syndrome) that independently raise risk.
- Such history lowers the threshold for surveillance and specialist referral.
Symptoms That Should Never Be Ignored
Early detection depends on recognizing warning signs and acting promptly.
Abnormal uterine bleeding
Any bleeding that is heavier, prolonged, or occurs between periods warrants evaluation. In PCOS patients, such bleeding may be the first sign that the endometrium has become hyperplastic.
Bleeding after menopause
Any postmenopausal bleeding is abnormal and requires urgent assessment — in Spain or elsewhere — because the probability of a pathologic process is higher.
Pelvic pain and pressure
Though less specific, persistent pelvic discomfort or unusual pelvic symptoms in a patient with PCOS should prompt clinical inquiry and often imaging.
PCOS, Infertility, and Endometrial Changes
Infertility in PCOS often reflects chronic anovulation; concurrently, the endometrium may undergo changes that both reflect and compound reproductive risks.
Endometrial hyperplasia explained
Endometrial hyperplasia is a spectrum of benign to atypical cellular proliferation of the uterine lining. In the context of PCOS, hyperplasia most commonly arises from chronic unopposed estrogen and can be detected by ultrasound (thickened lining) and confirmed by biopsy.
When hyperplasia becomes cancer
Atypical hyperplasia carries a measurable risk of progression to carcinoma if untreated. The goal of early detection and management is to reverse hyperplasia with hormonal therapy or to proceed to surgery only when necessary — strategies that preserve health and, when possible, fertility.
How Doctor Minig Diagnose Endometrial Cancer in PCOS Patients
Dr. Minig follows evidence-based steps to evaluate patients with PCOS and suspicious symptoms, balancing diagnostic accuracy with minimally invasive care.
Transvaginal ultrasound
Transvaginal ultrasound is the first-line imaging to measure endometrial thickness and investigate structural abnormalities. In PCOS patients, a persistently thickened endometrium on ultrasound prompts further diagnostic testing.
Endometrial biopsy
An endometrial biopsy provides tissue for histologic diagnosis. It is a minimally invasive, outpatient procedure that can detect hyperplasia, atypia, or carcinoma with high diagnostic value.
Hysteroscopy
Hysteroscopy allows direct visualization of the endometrial cavity and targeted sampling of suspicious areas. Specialists in Spain commonly use office or operative hysteroscopy when indicated for definitive diagnosis or directed treatment.
Why early testing saves lives
Early diagnostic steps allow clinicians to identify reversible or early-stage disease, apply medical therapies (for example, progestin treatment), and avoid progression. Prompt evaluation shortens time to treatment and can preserve fertility in many cases.
Treatment Options If Cancer or Precancer Is Found
Treatment is individualized to disease severity, patient age, fertility desires and comorbidities.
Hormonal treatment for early changes
Progestin therapy (systemic or intrauterine via a levonorgestrel IUD) is often effective in reversing non-atypical and some atypical hyperplasia. This approach is particularly relevant for women wishing to preserve fertility.
Surgical options
For confirmed endometrial carcinoma, standard treatment often involves hysterectomy with staging. Minimally invasive surgical approaches (laparoscopic or robotic) are widely used in Spain and reduce morbidity while maintaining oncologic outcomes.
Fertility-preserving approaches
In selected patients with early-stage, low-grade disease, conservative management with high-dose progestin and close surveillance can be considered under expert guidance. These decisions require multidisciplinary discussion and experienced gynecologic oncology teams.
Preventing Endometrial Cancer If You Have PCOS
Prevention focuses on reducing unopposed estrogen exposure and controlling metabolic contributors.
Regulating periods
- Inducing regular withdrawal bleeding (combined oral contraceptives or cyclic progestins) reduces endometrial buildup.
- For amenorrhea, scheduled progestin courses every 1–3 months are commonly recommended.
Weight and insulin control
- Lifestyle measures (diet, exercise) that reduce weight and improve insulin sensitivity substantially lower endometrial risk.
- Medical therapies (metformin) may assist metabolic control in many patients.
Role of progesterone therapy
Progesterone is protective of the endometrium; intrauterine systems (e.g., levonorgestrel IUD) provide targeted, long-term protection for many patients.
PCOS and Endometrial Cancer Care in Spain
Spain has strong specialist services for gynecologic oncology, accessible diagnostic pathways and a growing emphasis on minimally invasive, fertility-preserving care.
Why Spain is a trusted destination
Spain has specialized gynecologic oncology centers, experienced surgical teams, and widespread access to modern diagnostic and minimally invasive therapeutic technologies. For patients seeking high-quality care, Spain’s centers offer integrated diagnostics, fertility counseling and evidence-based treatment pathways.
Importance of seeing a gynecologic oncology specialist
Not all gynecologists manage cancer risk the same way. Specialist gynecologic oncologists — such as those in major Spanish centers and clinicians like Dr. Minig — can provide risk-stratified evaluation, fertility-preservation counseling and access to advanced surgical techniques.
The value of second opinions and expert care
Second opinions can be especially valuable when pathology is uncertain, when fertility preservation is desired, or when the treatment plan carries major long-term consequences. Seeking specialized input is a reasonable and recommended practice.
When Should You See a Doctor Immediately?
Early assessment changes outcomes — don’t delay evaluation when red flags appear.
Red-flag symptoms checklist
- No menstrual periods for several months with no medical management
- New or heavier vaginal bleeding
- Any vaginal bleeding after menopause
- Pelvic pain that is persistent or progressive
If you have any of these findings, consult a gynecologist or gynecologic oncologist promptly.
Living With PCOS Without Living in Fear
PCOS is manageable and risk can be reduced; informed monitoring is the practical response, not anxiety.
Monitoring vs panic
PCOS increases risk but does not determine fate. Regular monitoring, informed medical care, and sensible lifestyle measures keep most patients far from serious disease. Monitoring includes routine gynecologic follow-up, evaluation of menstrual patterns, and low threshold for imaging or biopsy when symptoms change.
Taking control of long-term health
Practical steps — regulating cycles, addressing weight and insulin resistance, and building a care team that includes an endocrinologist and gynecologist or gynecologic oncologist — dramatically reduce long-term risk and improve overall wellbeing.
Conclusion
PCOS does not cause endometrial cancer directly, but the chronic hormonal and metabolic environment it creates meaningfully increases endometrial risk if left unmanaged. The key clinical message is simple and actionable: recognize abnormal bleeding, regulate cycles, manage metabolic risk factors, and consult specialists early. In Spain, access to experienced gynecologic oncology teams and fertility-preserving treatment options (offered by clinicians such as Dr. Lucas Minig) makes early evaluation and personalized care realistic and effective.
FAQs
Can PCOS directly cause endometrial cancer?
No — PCOS is a risk factor because it commonly produces prolonged unopposed estrogen exposure, which can lead to endometrial hyperplasia and, in some cases, cancer over time.
Do all women with PCOS need endometrial biopsies?
Not routinely. Biopsy is indicated when there are symptoms (abnormal bleeding), a persistently thickened endometrium on ultrasound, or other clinical concerns. Decisions are individualized.
Can endometrial cancer be prevented in PCOS patients?
Often yes. Period regulation (hormonal contraception or cyclic progestins), weight management, and treating insulin resistance are effective preventive strategies.
Is endometrial cancer common in young women with PCOS?
It is uncommon in young women but not impossible, particularly with long periods of untreated anovulation. Persistent abnormal bleeding warrants prompt evaluation regardless of age.
Should I see a gynecologic oncology specialist in Spain if I’m worried?
If you have prolonged menstrual irregularity, abnormal bleeding, or a biopsy/ultrasound finding of concern, a specialist consultation (as provided by experienced clinicians in Spain, including Dr. Minig’s practice) is appropriate to evaluate risk and plan management.