Discover how transvaginal ultrasound can spot warning signs of endometrial cancer, its limits, and Dr. Lucas Minig’s fast diagnostic pathway in Spain. Get clear answers & book a consultation.
Introduction
Transvaginal ultrasound (TVUS) is one of the most frequently used imaging tests when clinicians evaluate the uterus and its lining. For patients and clinicians alike, a central question surfaces repeatedly: can endometrial cancer be detected by ultrasound? The short, practical truth is that ultrasound is an excellent triage tool — it identifies suspicious changes such as endometrial thickening, focal masses, or intrauterine fluid — but it does not replace tissue diagnosis.
This document explains, in patient-centered detail, what ultrasound can and cannot reveal about the endometrium, how clinicians interpret findings, what the next steps are when imaging is suspicious, and how these pathways are commonly managed in Spain by specialist teams (including practices such as Dr. Lucas Minig’s at IMED Valencia).
Table of Contents
Can endometrial cancer be detected by ultrasound?
Yes — ultrasound (especially transvaginal ultrasound, TVUS) can detect signs that may suggest endometrial cancer, such as a thickened uterine lining or a visible mass. However, ultrasound cannot definitively diagnose endometrial cancer. To confirm a diagnosis, a tissue sample (an endometrial biopsy or a hysteroscopy-guided biopsy) is required.
Why ultrasound is often the first test ordered?
Doctors order ultrasound first because it’s quick, non-invasive, widely available, and gives useful information about the uterus and endometrium. Think of it as the “first look” — it tells the clinician whether there’s reason to investigate further. In many clinics across Spain and worldwide, a transvaginal ultrasound is the preferred starting point when a patient reports abnormal vaginal bleeding or other related symptoms.
What is transvaginal ultrasound (TVUS) and how does it work?
A transvaginal ultrasound (TVUS) uses a small probe inserted into the vagina to send sound waves into the pelvis and create high-resolution images of the uterus, endometrium (uterine lining), and ovaries. Because the probe is closer to the organs, TVUS gives much clearer detail than an abdominal (pelvic) ultrasound.
TVUS vs abdominal ultrasound: why approach matters
- Abdominal ultrasound is performed over the lower belly. It’s useful for large structures and general pelvis anatomy, but it’s limited by body habitus (for example, in people with higher BMI) and bladder filling.
- Transvaginal ultrasound (TVUS) provides a close-up, “macro lens” view of the endometrium and uterine cavity. For endometrial concerns, TVUS is almost always the better choice.
Which approach is used depends on symptoms, patient comfort, and what the clinician needs to see. Most clinics in Spain use TVUS as the routine first-line test when endometrial pathology is suspected.
What TVUS images show (endometrial lining, masses, fluid)?
TVUS images let the sonographer or gynecologist measure:
- Endometrial thickness (in millimetres),
- Focal masses or polyps inside the uterine cavity,
- Fluid in the uterine cavity (sometimes a sign of bleeding or other issues),
- Irregularities of the endometrial surface, and
- Blood flow patterns if Doppler imaging is used.
These visual clues help doctors decide whether further sampling (biopsy) or targeted procedures are needed.
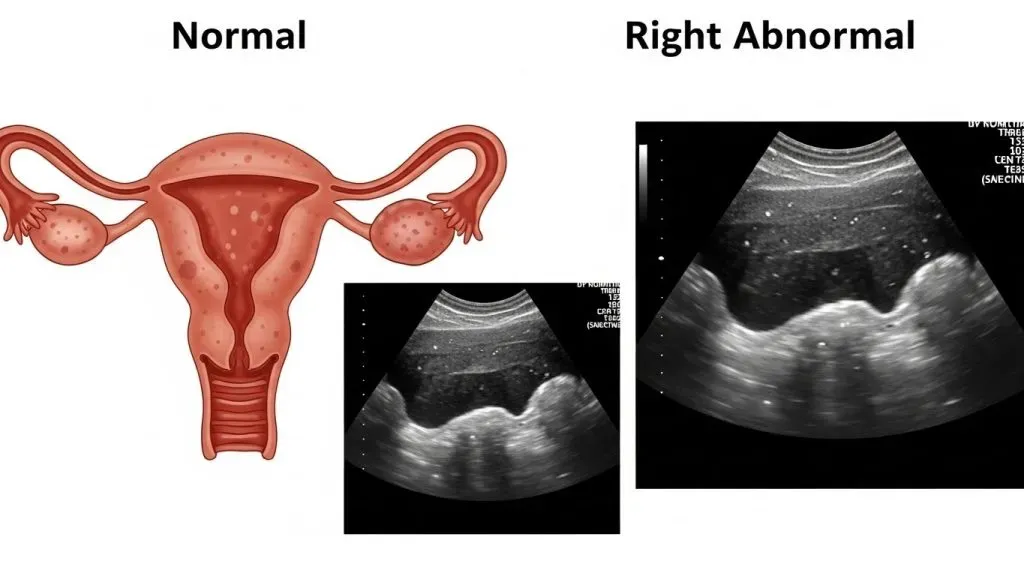
What ultrasound can show about the endometrium?
Ultrasound is a structural test: it shows shape, size, and some functional indicators (like blood flow) — not the microscopic make-up of the tissue. Here’s what it commonly reveals.

Endometrial thickness: the first red flag
One of the most important ultrasound findings is the thickness of the endometrium. In general:
- A thin lining in a postmenopausal woman usually lowers suspicion for cancer.
- A thickened lining raises concern and typically triggers a biopsy.
The exact numeric cut-off varies by guideline and clinical context, but the concept is consistent: thickness matters, especially in people after menopause.
Masses, polyps and suspicious shapes on ultrasound
TVUS can spot focal masses or polyps inside the uterine cavity. While seeing a mass is important information, ultrasound alone cannot reliably tell whether a mass is benign (like a polyp) or malignant (cancer). That’s why a suspicious mass usually leads to targeted removal or biopsy.
Doppler and 3D features that add detail
Advanced ultrasound techniques — Doppler (assessing blood flow) and 3D imaging — can provide additional clues. Tumours often have different vascular patterns than benign lesions. Combining these features with thickness and morphology improves diagnostic confidence, although it still doesn’t replace a tissue diagnosis.
What ultrasound cannot do — why it’s not definitive?
Benign vs malignant: the limits of imaging
Ultrasound shows what is there, not what the cells are like. A thick endometrium can be:
- cancer,
- benign hyperplasia (non-cancer growth),
- a polyp,
- or related to hormonal treatments.
Only microscopic examination of a biopsy sample can determine the presence of cancer cells. So ultrasound is a guide — not a final answer.
False positives and false negatives — real-life examples
- False positive: A postmenopausal patient has a thickened lining on TVUS but biopsy reveals benign polyp or hormonal change. The scan raised alarm unnecessarily but led to appropriate reassurance.
- False negative: A thin lining is measured on ultrasound but the patient still has cancer — rare, but possible in specific clinical contexts. That’s why symptoms and risk factors are always considered alongside imaging.
These possibilities underline why doctors combine clinical judgment, imaging, and tissue sampling.
How accurate is ultrasound for detecting endometrial cancer? (sensitivity & specificity)?
Ultrasound accuracy varies by population, the thickness threshold used, and whether advanced features (Doppler/3D) are included. Broadly:
- TVUS is sensitive for picking up structural abnormalities, particularly in symptomatic postmenopausal women.
- Specificity (ability to rule out non-cancer) varies — meaning ultrasound sometimes flags benign conditions as suspicious.
Clinical practice typically balances sensitivity and specificity by choosing a thickness cut-off and combining ultrasound appearance with symptoms and risk factors.
Thresholds (4–5 mm, 6–8 mm) and what they mean
Common clinical thresholds include:
- 4–5 mm: Often used in symptomatic postmenopausal women as a conservative threshold — a lining ≤4–5 mm makes cancer unlikely and may avoid urgent biopsy unless symptoms persist.
- 6–8 mm: Used in some contexts (premenopausal women, women on hormone therapy) where the lining may normally be thicker; these higher thresholds increase specificity but may lower sensitivity.
These thresholds are tools for decision-making; they aren’t absolute rules.
Algorithms and scoring systems (REC-score) that improve accuracy
To improve diagnostic performance, researchers and clinicians sometimes use scoring systems that combine:
- endometrial thickness,
- Doppler vascular patterns,
- patient risk factors (age, BMI, bleeding history).
These algorithms can sharpen the assessment and guide who needs urgent biopsy versus monitoring. Still, biopsy remains the defining diagnostic step.
When should you get a TVUS? Symptoms that matter?
Postmenopausal bleeding: the single most important sign
If you’ve gone through menopause, any vaginal bleeding is a red flag and should prompt a clinical evaluation, typically including TVUS. Most endometrial cancers are detected because of bleeding, which makes this symptom crucial.
Abnormal uterine bleeding in premenopausal women
Heavy or irregular bleeding, bleeding between periods, or bleeding that doesn’t respond to standard treatment also warrants evaluation. Age, medical history (obesity, diabetes, tamoxifen use, hereditary risk like Lynch syndrome), and exam findings inform how urgently a scan is done.
If ultrasound is suspicious — next diagnostic steps
If TVUS shows a thickened endometrium, a mass, or other worrying features, doctors typically move to tissue sampling and more detailed imaging.
Endometrial biopsy (pipelle) — the gold standard
A pipelle biopsy is an office procedure that samples the endometrial lining. It’s quick, low-risk, and provides tissue for pathology. A positive biopsy confirms cancer; a negative biopsy may still be followed by further testing if suspicion remains.
Hysteroscopy-guided biopsy and D&C
Hysteroscopy lets the doctor directly view the uterine cavity and take targeted biopsies — ideal for focal lesions or when the pipelle didn’t get a good sample. Dilation and curettage (D&C) may be used if office sampling isn’t feasible.
MRI and other imaging for staging
If cancer is confirmed, MRI is usually ordered to assess the depth of myometrial invasion and check for spread — critical information for surgical planning. Ultrasound gives clues about invasion but MRI provides more accurate staging.
How doctors in Spain manage suspicious ultrasound findings?
Typical pathway in Spanish hospitals / private clinics
In Spain, pathways are similar to best practices worldwide: clinical evaluation → TVUS → if abnormal, pipelle or hysteroscopy → pathology review → MRI for staging if cancer is confirmed → multidisciplinary team planning treatment. Large public hospitals and private clinics often offer rapid access programs so symptomatic patients don’t wait long for tests.
What a specialist like Dr. Lucas Minig offers (fast triage, minimally invasive approach)?
Specialist clinics in Spain — for example in Valencia — often provide accelerated diagnostic services: quick teleconsultations, targeted TVUS review, same-week pipelle or hysteroscopy, and fast pathology turnaround. Surgeons like Dr. Lucas Minig focus on minimally invasive treatment options (laparoscopy, robotic surgery) that aim to reduce hospital stay and speed recovery, while also offering clear communication and patient-centred care throughout the process.
What to bring to your appointment and how to prepare?
Records, prior scans, symptoms diary
Bring:
- Any previous ultrasound or MRI images (digital files or CDs are helpful),
- Prior pathology reports,
- A short timeline of symptoms (when bleeding began, pattern, any treatments tried),
- A list of medications (like tamoxifen or hormone therapy).
Having these saves time and helps your doctor avoid repeating tests.
Questions to ask your doctor (short checklist)
- What did the ultrasound show exactly (measurement and description)?
- Do I need a pipelle biopsy or hysteroscopy?
- What are the possible causes of this ultrasound finding?
- If cancer is diagnosed, what are my treatment options here in Spain?
- How quickly can I get the next test and results?
Bring a notebook or use your phone to record answers — it’s easy to forget details in clinic.
Practical patient tips: interpreting results without panic
How to read “thickened endometrium” on a report
If your report says “thickened endometrium,” ask for the numeric measurement (e.g., 7 mm). A number gives a clearer sense of risk than the word “thickened.” Many thickened linings turn out to be benign, but follow-up is important to be safe.
When to seek a second opinion
Seek a second opinion if:
- The results and plan are unclear,
- You’re told nothing further is needed despite ongoing bleeding,
- You simply want reassurance from a specialist (common and reasonable).
Specialist centres in Spain often offer second-opinion services and rapid reassessment.
Ultrasound in screening vs diagnosis: why we don’t screen everyone
Routine ultrasound screening of asymptomatic women is not recommended because it hasn’t been shown to reduce deaths from endometrial cancer and may lead to unnecessary invasive procedures. Instead, ultrasound is a targeted diagnostic tool used when symptoms or risk factors raise concern.
Evidence & guidelines (why screening is not routine)
Because the most common early symptom — abnormal bleeding — tends to appear before advanced disease develops, targeted evaluation of symptomatic women is the most effective strategy. Population-level screening would produce many false positives and unnecessary biopsies without a clear survival benefit.
FAQ’s
Can a normal transvaginal ultrasound completely rule out endometrial cancer?
No test is 100% perfect, but a thin endometrium (commonly ≤4–5 mm in symptomatic postmenopausal women) makes cancer very unlikely. Persistent symptoms should still be investigated.
If my ultrasound shows a polyp, does that mean I have cancer?
Most uterine polyps are benign. A suspicious-looking polyp is usually removed or biopsied to confirm whether it contains abnormal cells.
How soon should I get a biopsy after a suspicious ultrasound?
Timing depends on local services and your symptoms, but many clinics aim to complete biopsy within days to weeks for symptomatic patients. Specialist centres in Spain often offer accelerated scheduling.
What happens if my biopsy is negative but ultrasound looks worrying?
If a pipelle biopsy is non-diagnostic or negative but suspicion remains high, hysteroscopy with targeted biopsy is usually the next step.
Can ultrasound tell how advanced endometrial cancer is?
Ultrasound can suggest whether a tumour invades deeply, but MRI provides more accurate staging information for surgical planning.
Conclusion
Ultrasound — especially transvaginal ultrasound — is a powerful, accessible first step to detect signs that may point to endometrial cancer. It’s fast, non-invasive, and excellent at showing the structure of the uterine lining. But ultrasound is a detecting tool, not a diagnosing tool: only a biopsy can tell whether abnormal cells are cancerous.
If you’re in Spain and worried about abnormal bleeding or a suspicious ultrasound, ask for a focused, specialist-led pathway that includes prompt biopsy and, if needed, staging and minimally invasive treatment. Clear communication, quick action, and careful follow-up are the priorities — and they can make all the difference.