Most endometrial cancers are not inherited. Learn when genetics matters, how Lynch syndrome is tested, and how Dr. Minig’s team in Spain can help — book a consult.
Introduction
Endometrial cancer — cancer of the uterus lining — raises a common and urgent question: is it passed down in families? The truth is nuanced. Below you’ll find a practical, patient-friendly breakdown of what “genetic” means in this setting, which inherited syndromes matter, how doctors test, and what to ask your clinician in Spain. I also explain how specialists such as Dr. Lucas Minig typically handle genetic risk in clinical practice.
Is Endometrial Cancer Genetic?
Most endometrial cancers are not inherited, but a minority are caused by germline (inherited) mutations — and identifying those changes can be vital for your treatment, follow-up and family members. A single inherited syndrome, Lynch syndrome, is the most important hereditary cause to know about.
How most endometrial cancers start?: sporadic vs. hereditary
Most cases begin because of DNA changes that happen during a person’s life; a smaller but clinically significant group arise from mutations you inherit.
Somatic (non-hereditary) mutations: common drivers
Somatic mutations develop in endometrial cells over time. These mutations are limited to the tumour tissue and are driven by aging, hormonal exposure, obesity, diabetes and other environmental or metabolic risks. Somatic changes explain the majority of endometrial cancer cases and are the reason many tumours are single, isolated events in a person’s life.
Germline (inherited) mutations: a smaller but important group
Germline mutations are present in every cell from birth and can be passed to children. While they account for a minority of cases, their detection matters because they change how clinicians screen patients and family members — often prompting earlier surveillance and cascade testing for relatives. For endometrial cancer, Lynch syndrome is the principal hereditary cause.
What Does “Genetic” Really Mean in Cancer?
In oncology, the label “genetic” can mean two different things: an acquired change inside the tumour or an inherited mutation carried in every cell. Knowing which you’re dealing with guides management.
Inherited (Germline) Mutations
These are mutations you were born with. They may dramatically raise lifetime cancer risk for you and can be passed on to children. Identification requires germline genetic testing (blood/saliva) and genetic counselling to explain implications for the patient and relatives. Lynch syndrome and Cowden syndrome are examples of germline conditions that raise endometrial cancer risk.
Acquired (Somatic) Mutations
Somatic mutations occur only within the tumour. They are not passed to family members. Tumour sequencing or specific tumour tests (like IHC or MSI) detect these changes and can also suggest whether germline testing is needed.
Why This Difference Matters for Families?
If a mutation is germline, relatives may have a higher risk and benefit from targeted screening or preventive measures. If it’s somatic, actions focus on the patient’s treatment and prognosis without the same family cascade implications.
The Main Hereditary Cause: Lynch Syndrome
Lynch syndrome is central when discussing hereditary endometrial cancer because it both increases risk and is relatively more common than other inherited causes.
What Is Lynch Syndrome?
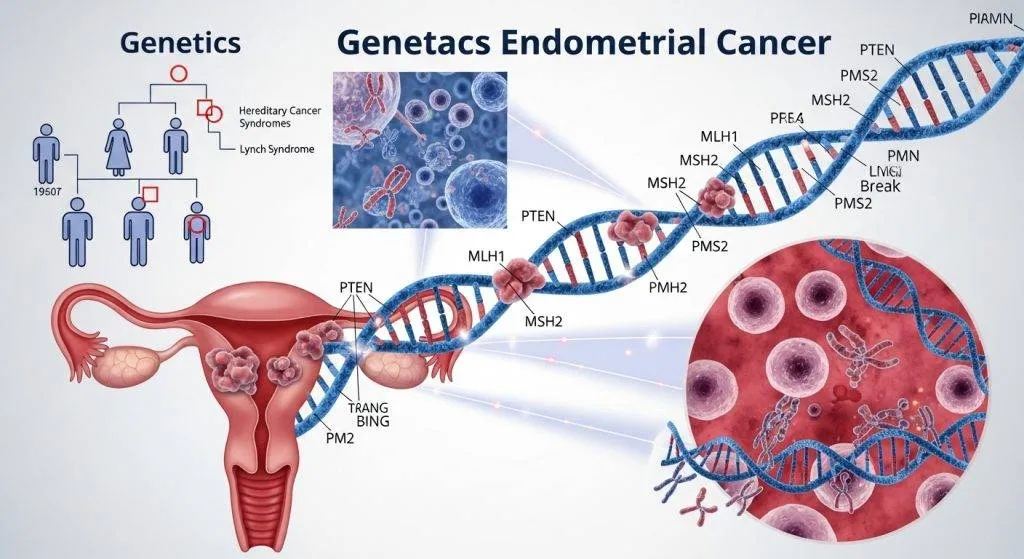
Lynch syndrome is an inherited condition caused by pathogenic variants in DNA mismatch repair (MMR) genes that normally correct replication errors. People with Lynch have higher lifetime risks of several cancers, most notably colorectal and endometrial cancers. Detection allows targeted surveillance for relatives and personalized management for the patient.
Mismatch Repair (MMR) Genes Explained
Key genes include MLH1, MSH2, MSH6, PMS2 (and sometimes deletions affecting EPCAM). When these fail, the tumour often shows microsatellite instability (MSI) or absence of MMR proteins on immunohistochemistry (IHC), both of which are flagged by pathology labs and used to guide further testing. Universal tumour screening strategies use IHC/MSI as the first triage step.
Lifetime Risk in Women with Lynch Syndrome
Estimates vary by gene and study, but women with Lynch carry substantially increased lifetime risks of endometrial cancer — frequently cited ranges are roughly 40–60% for some mutation carriers, and some series report wider ranges depending on gene and population. Detection dramatically changes surveillance recommendations.
Other Genetic Syndromes Linked to Endometrial Cancer
Lynch is the most important, but other inherited conditions also elevate risk — though they are rarer.
Cowden Syndrome (PTEN Mutation)
Cowden syndrome (caused by PTEN mutations) increases the lifetime risk of several cancers, including endometrial cancer (estimates commonly quoted around 5–10% lifetime risk for endometrial cancer). Patients with features of Cowden (mucocutaneous lesions, macrocephaly, family history) should be evaluated by genetics.
BRCA and Rare Genetic Associations
BRCA1/2 carriers are primarily at elevated risk for breast and ovarian cancer; some studies suggest a small increase in endometrial cancer risk, particularly certain aggressive histologies, but BRCA is not a major driver of endometrial cancer overall. Other ultra-rare syndromes may appear in selected families.

How common is genetic endometrial cancer? (numbers & context)
Population studies and systematic reviews suggest that Lynch explains roughly ~3% of endometrial cancers in many cohorts; when you include rarer syndromes, the hereditary fraction increases modestly but remains a minority. Differences in estimates arise from population genetics and whether universal tumour screening is implemented. These numbers support routine tumour triage (IHC/MSI) to pick up potential hereditary cases efficiently.
Who should be evaluated for hereditary risk? (practical checklist)
Most centres now use tumour-first screening, but certain clinical flags still prompt genetic referral.
Age and family history red flags
- Endometrial cancer diagnosed under age 50
- Personal history of colorectal cancer or multiple Lynch-associated tumours
- Family history of early colorectal or endometrial cancer (first- or second-degree relatives)
If these fit you, ask for genetic counselling.
Tumor testing that points to Lynch: IHC and MSI
Loss of MMR proteins on IHC or high MSI on tumour testing signals possible Lynch syndrome and triggers germline testing unless attributable to a non-hereditary cause (e.g., MLH1 promoter hypermethylation). Pathology triage is a standard, evidence-based route to decide who needs germline testing.
What tests are used (tumor tests, germline panels) and how testing works in Spain?
In clinical practice the pathway typically begins in pathology and then moves to genetics.
IHC / MSI tumor tests
Pathology uses IHC to check for MMR protein expression and/or molecular MSI testing. These are performed on tumour tissue and are quick ways to flag MMR deficiency. If IHC shows MLH1 loss, labs usually test for MLH1 promoter methylation to separate sporadic methylation from Lynch-related loss.
Germline genetic testing and panels
If tumour testing suggests Lynch (or if family history indicates), patients are referred for germline testing via blood or saliva. Modern panels test MMR genes and other relevant genes (e.g., PTEN, POLE) depending on clinical context. Genetic counsellors explain implications, consent, and arrange cascade testing for relatives if a pathogenic variant is found.
Does a Family History Mean You Will Get Cancer?
Not necessarily. A family history raises suspicion and may increase personal risk, but it does not guarantee that you will develop cancer. Testing clarifies whether a shared inherited mutation explains the family pattern — and if not, other factors (shared environment, chance) may be at play. Genetic counselling helps patients interpret risk realistically.
If a hereditary mutation is found: what changes for the patient and family
Finding a pathogenic germline variant changes follow-up and prevention strategies for both the patient and at-risk relatives.
Surveillance and risk-reducing options
For Lynch carriers, surveillance may include earlier and more frequent colonoscopies, consideration of risk-reducing hysterectomy (after childbearing), and tailored imaging or blood markers. Each plan is individualized based on gene, age, family plans, and comorbidities.
Family cascade testing
Relatives can be offered targeted testing for the identified familial mutation. This cascade testing is a powerful prevention tool: relatives who test positive can follow intensified surveillance or preventive options; those who test negative may avoid unnecessary interventions.

Treatment Implications of Genetic Endometrial Cancer
A genetic diagnosis can influence both immediate and long-term management.
Immunotherapy and Targeted Treatments
Tumours with MMR deficiency / high MSI may respond to immune checkpoint inhibitors, an important therapeutic consideration for advanced or recurrent disease. Thus, MMR/MSI testing serves both hereditary and therapeutic purposes.
Personalized Oncology in Spain
In Spain, gynecologic oncology teams integrate molecular and genetic findings into surgical, medical and surveillance plans. Multidisciplinary boards (including genetics, pathology, oncology and gynaecologic surgery) help tailor treatment — something experts such as Dr. Lucas Minig routinely participate in for complex cases.
Practical pathway in Spain (how patients typically get tested and treated)
In Spain most hospitals — public and private — now incorporate tumour MMR/MSI testing for endometrial cancer or have clear referral routes to genetics units. If tumour tests suggest an inherited cause, patients are referred to a clinical genetics service and to a gynecologic oncologist for personalized care. Private clinics and labs also provide germline panels and rapid consultations.
Who should be referred to genetic counselling?
- Patients under 50 with endometrial cancer
- Tumour shows MMR deficiency without clear sporadic cause
- Strong family history of Lynch-related cancers
Referral pathways vary by centre, but asking your treating physician or contacting a genetics unit starts the process.
Local services, labs and hospital links
Large Spanish oncology departments and private networks (university hospitals, specialized cancer centres and reputable genetic labs) offer the full pathway — from tumour testing to germline panels and counselling. If you prefer a fast specialist opinion, experienced gynecologic oncologists such as Dr. Lucas Minig can advise on testing priorities, surgical options and referrals.
When to ask your doctor: checklist for patients?
- Has my tumour been tested for MMR or MSI?
- Did pathology test MLH1 methylation if MLH1 was lost?
- Do I meet criteria for germline genetic testing?
- Can I get a genetic counselling referral and a second opinion with a gynecologic oncologist?
- What will a positive result mean for my relatives?
Bring this checklist to your appointment — it helps focus the conversation and speeds decision-making.
How Dr. Lucas Minig and specialists approach genetic risk?
Clinicians like Dr. Lucas Minig emphasize rapid, patient-centred triage: order tumour IHC/MSI early, explain results in plain language, and refer promptly to genetics when indicated. Dr. Lucas Minig frequently coordinates between pathology, genetics and surgery to ensure patients in Valencia and beyond get a coherent, evidence-based plan that covers treatment and family protection.
Common myths and clear facts
- Myth: “If one relative had endometrial cancer, the whole family is doomed.”
Fact: Family history raises suspicion but testing tells the story. - Myth: “Only colon cancer matters for Lynch.”
Fact: Lynch also strongly raises endometrial cancer risk; for some women it’s the first cancer diagnosed. - Myth: “Genetic testing is experimental.”
Fact: Tumour triage and clinical germline testing are standard, guideline-backed steps in modern care.
FAQs
How often is Lynch syndrome the reason for endometrial cancer?
Many studies put Lynch prevalence in endometrial cancer cohorts at roughly ~3%, though estimates vary; this supports routine tumour screening to avoid missed cases.
If my tumour is MMR-deficient, does that always mean I have Lynch?
Not always — some tumours lose MMR function due to somatic events (like MLH1 promoter methylation). The pathology team will typically test for methylation and, if suspicion persists, refer for germline testing.
Can finding a hereditary mutation change my treatment?
Yes. MMR-deficient tumours may respond to immunotherapy, and knowledge of a mutation informs surveillance and risk-reducing options for you and relatives.
What other syndromes should I know about besides Lynch?
Cowden syndrome (PTEN mutations) raises endometrial cancer risk, and rare links with BRCA or polymerase proofreading defects exist; the context determines testing choices.
I live in Spain — what are the next practical steps?
Ask your treating team whether tumour IHC/MSI was performed. If not, request it. If results suggest MMR deficiency or you have an early onset/family history, ask for a genetics referral or a specialist opinion from a gynecologic oncologist such as Dr. Lucas Minig.
Conclusion
So, is endometrial cancer genetic? Usually not — most cases are sporadic — but a meaningful minority are hereditary, primarily due to Lynch syndrome and, less commonly, other syndromes like Cowden. The practical workflow is clear: tumour IHC/MSI → genetic counselling → germline testing when indicated → individualized surveillance and family testing. If you live in Spain and are navigating this process, ask your treating team about MMR/MSI testing or seek a specialist opinion; gynecologic oncologists such as Dr. Lucas Minig provides integrated care that links testing with treatment and family protection.