Wondering how long radiation treatment for endometrial cancer takes? Get clear timelines for EBRT, brachytherapy, and combined treatment—what to expect day-to-day and how to plan.
Introduction
When you hear that radiation therapy is part of your endometrial cancer treatment plan, one of the first questions that naturally comes to mind is: How long will this last? Understanding the timeline helps you prepare mentally, physically, and practically — especially if you are coordinating care in Spain or traveling for treatment.
Radiation treatment for endometrial cancer is carefully structured, but the total duration varies depending on the type of radiation, the stage of the disease, and individual medical factors. Let’s break it down clearly and realistically.
How Long Is Radiation Treatment for Endometrial Cancer?
In most cases, radiation treatment lasts between one and six weeks, but the exact duration depends on the technique used and the clinical situation.
Average duration overview
For many women:
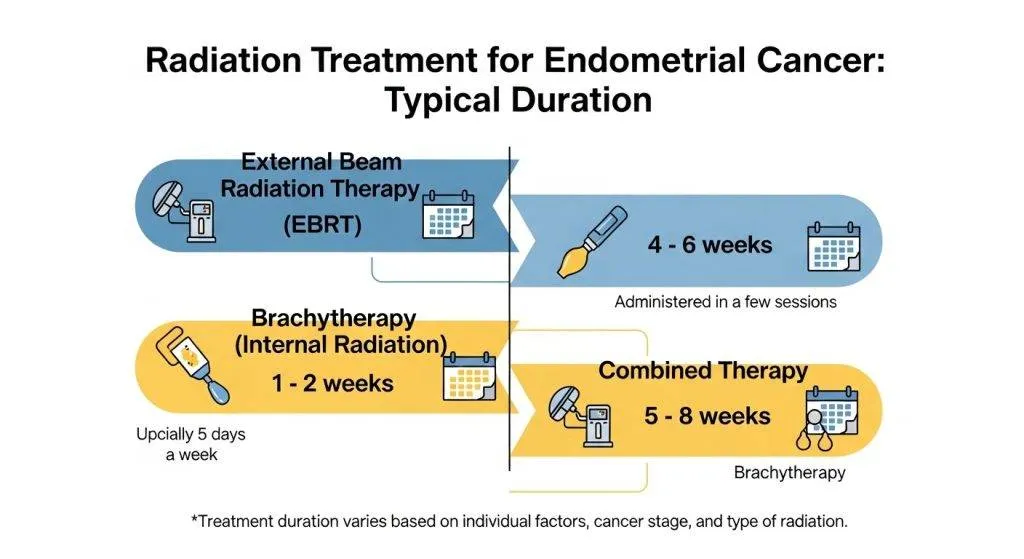
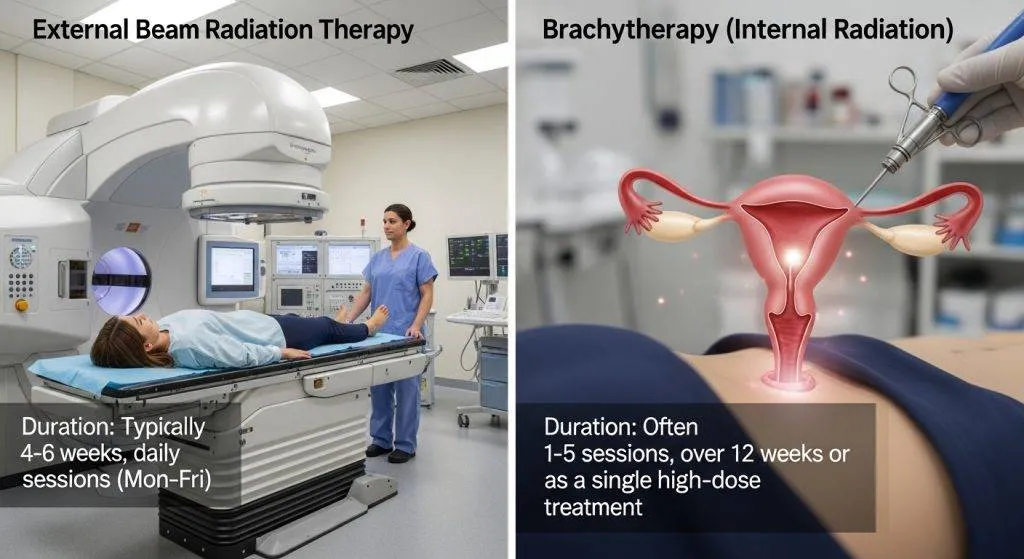
- External Beam Radiation Therapy (EBRT) typically runs 4–6 weeks, delivered five days per week.
- High-Dose-Rate (HDR) brachytherapy usually takes 1–3 weeks, with a few short sessions.
- When both are combined, the overall timeline can extend to 6–8 weeks including planning and recovery.
These timeframes are standard in many oncology centers in Spain and across Europe.
Why there is no single timeline
There isn’t a one-size-fits-all schedule because the plan is tailored to tumor stage, grade, pathology results after surgery, whether chemotherapy is combined, and patient-specific factors such as recovery speed and comorbidities. In practice, the radiation oncologist designs the fractionation (dose per session) and total sessions to balance tumor control with side-effect risk.
Types of radiation used for endometrial cancer
External beam radiation therapy (EBRT)
EBRT uses focused radiation beams from outside the body to treat the pelvis. It’s used when risk extends beyond the uterus — for example, if lymph nodes may be involved or deep myometrial invasion is present. EBRT is planned with CT (and sometimes MRI) simulation to shape beams precisely and spare normal tissues.
Brachytherapy (HDR and LDR)
- HDR (High-Dose-Rate) brachytherapy: A highly targeted internal radiation delivered via an applicator placed in the vagina. The radiation source is active for a short time (minutes) and removed each session. HDR is the most common brachytherapy approach for endometrial cancer because it’s efficient and usually outpatient.
- LDR (Low-Dose-Rate) brachytherapy: A continuous low-dose source may be implanted for hours to days. LDR is less used for routine endometrial adjuvant therapy today but still relevant in some centers or specific clinical situations.
Combined approaches and when each is used
- EBRT alone may be chosen for patients with more extensive pelvic risk.
- Brachytherapy alone is common for early-stage, low-risk disease where local (vaginal cuff) control is the main goal.
- EBRT + brachytherapy is used when both pelvic fields and a local boost are needed — for example, higher-risk histology or nodal involvement.
Your radiation oncologist will explain why a combined plan is recommended and what that means for the overall duration.
Typical treatment timelines
Below are common schedules used in many centers.
EBRT schedules (fractionation and total weeks)
- Standard fractionation: 1 fraction/day, 5 days/week, for about 4–6 weeks (≈ 20–30 fractions).
- Each daily visit: usually 15–45 minutes in the department; machine “beam-on” time is only a few minutes.
This schedule balances effectiveness and normal tissue tolerance and is still the backbone of many adjuvant plans.
HDR brachytherapy schedules (sessions and spacing)
HDR schedules vary, but typical regimens include 2–5 sessions, often delivered as 3 fractions over 1–3 weeks (for example, 3 sessions spaced one week apart). Each session takes only minutes for dose delivery, though preparation and recovery make the visit closer to 30–60 minutes.
LDR brachytherapy (hospital stays)
LDR is uncommon but used in select cases. It typically requires 1–4 days of continuous delivery with inpatient monitoring. Because LDR ties patients to the hospital for multiple days, most centers now prefer HDR when appropriate.
Hypofractionation and shorter-course options
Hypofractionation (larger doses per session over fewer visits) is increasingly used in carefully selected patients. For some patients this can shorten EBRT to 3–4 weeks. Not every patient is a candidate — oncologists weigh tumor size, nearby organs, and long-term toxicity risk before choosing this approach.
What determines how long radiation lasts?
Stage and grade of the tumor
Early-stage, low-grade cancers may require only vaginal brachytherapy. Higher-stage disease or high-grade histology is more likely to need pelvic EBRT ± brachytherapy.
Treatment intent: adjuvant, definitive, palliative
Adjuvant radiation (after surgery) aims to reduce recurrence risk and follows typical fractionation. Definitive radiation (rare for endometrial cancer when surgery isn’t possible) and palliative radiation (to relieve symptoms) use different dose strategies and timelines geared to the goal of care.
Patient health, concurrent treatments, and logistics
Concurrent chemotherapy may be given with radiation in some scenarios; this can affect tolerance and scheduling. Severe comorbidities, healing after surgery, or need for travel/logistics can also shape the timetable.
What a typical week looks like during radiation
This prepares you for the rhythm of treatment days.
Daily appointment flow
- Check-in & vitals (brief): nurse visit for symptom check and any weight or hydration needs.
- Positioning & setup: therapists ensure you’re in the exact same position as during simulation (tattoos/marks).
- Imaging/verification: quick x-ray or cone-beam CT to confirm alignment.
- Treatment delivery: beam is on for a few minutes.
- Post-treatment: brief check with staff if any acute issues are present.
Expect to be at the center 20–45 minutes per EBRT session; brachytherapy days are often shorter for the active dose but may include additional prep time.
Symptoms week-by-week
- Week 1: many patients feel fine or slightly tired. Bowel/bladder irritation is usually minimal.
- Weeks 2–4: fatigue often increases; urinary frequency, mild diarrhea or rectal urgency may appear. Skin in the treated field can become irritated.
- Week 5–6 (if on EBRT): symptoms often peak near the end of treatment.
- After completion: acute symptoms usually begin to improve within 2–6 weeks, but fatigue can linger longer.
Side effects and how long they last
A simple orientation to acute vs late effects and management.
Acute effects (during and immediately after treatment)
- Fatigue: common, peaking late in the course and improving over weeks-months.
- Urinary symptoms: frequency, urgency, burning — typically resolve within weeks after treatment.
- Bowel symptoms: loose stools, cramping — often manageable with diet and medication.
- Vaginal changes: dryness, irritation — brachytherapy may cause local effects that improve with time and local care.
Late effects (months to years after)
Less commonly, radiation can cause long-term changes such as vaginal stenosis, chronic bowel or urinary symptoms, or pelvic discomfort. These late effects may appear months or years later; proactive follow-up and early intervention help reduce their severity.
Practical tips to manage side effects
- Stay hydrated and eat small frequent meals if bowel symptoms arise.
- Use prescribed topical agents and follow sexual health guidance after brachytherapy to minimize stenosis.
- Rest and prioritize gradual return to activity; listen to your body.
- Keep open communication with your radiation nurse/oncologist — early symptom control prevents treatment breaks.
Timing: when radiation starts after surgery
There is no one-size-fits-all waiting period, but typical practice is to allow sufficient wound healing — often 2–8 weeks after hysterectomy — before starting adjuvant radiation. Starting too early can risk wound complications; starting too late may slightly affect the theoretical benefit of adjuvant therapy. Multidisciplinary teams aim to find a safe, evidence-based window for each patient.
Technologies that can shorten treatment time
Advanced planning, image guidance, and stereotactic techniques allow for more precise targeting and occasionally enable hypofractionated approaches (fewer sessions). However, these decisions are clinical — precision does not always equate to fewer sessions for endometrial cancer because tolerance of nearby organs must guide dosing.
Decision-making: how doctors choose the schedule
Multidisciplinary team inputs
Radiation decisions come from tumor boards where gynecologic surgeons, radiation oncologists, medical oncologists, radiologists, and pathologists review each case together. This ensures the plan meshes with surgery and systemic therapy.
Patient preferences and shared decision-making
Doctors consider your lifestyle, travel ability, and personal priorities. Shared decision-making balances the scientific rationale with what is realistic and tolerable for you.
Dr. Lucas Minig — How Dr. Lucas coordinates radiation care
Credentials and clinical approach
Dr. Lucas Minig emphasizes clear communication and coordination. He reviews pathology and surgical reports personally to ensure radiation oncologists receive complete information for an optimal plan.
How he works with radiation oncologists
He participates in multidisciplinary reviews and communicates directly with radiation teams to align timing, indicate surgical findings that affect target volumes, and advocate for patient-friendly schedules where medically appropriate.
How his clinic supports travel, scheduling, and follow-up
Dr. Lucas’s practice often helps patients arrange appointments, advise on hypofractionation candidacy, and set up follow-ups to monitor recovery — a useful asset for patients traveling from other regions.
Follow-Up After Radiation Treatment Ends
Monitoring schedule
Follow-up typically begins 4–6 weeks after treatment, then every 3–6 months for the first 2 years, tapering to annual visits. These visits check symptoms, exam findings, and any late effects.
Long-term recovery and surveillance
Recovery is gradual. Energy and acute side effects often improve over months; surveillance focuses on symptom review and periodic imaging only when clinically indicated.
FAQs
How long will each radiation clinic visit take?
Most visits are 20–40 minutes: positioning and imaging (5–15 minutes), radiation delivery (2–5 minutes), plus check-in and any brief nursing assessment.
Can I combine radiation with chemotherapy?
In selected cases yes; concurrent chemo-radiation may be recommended for high-risk disease. This changes monitoring and sometimes symptom intensity, and the schedule is individualized.
Is it safe to travel during treatment?
Daily EBRT makes travel difficult. Short trips during brachytherapy weeks are often possible. Discuss travel plans with your team — many clinics help arrange lodging if needed.
How should I prepare on the day of brachytherapy?
Follow fasting or bowel prep instructions if given, bring a list of meds, and expect brief discomfort during applicator placement. Ask about analgesia or sedation options.
When should I contact my care team during radiation?
Report new or worsening symptoms (fever, severe diarrhea, uncontrolled urinary burning, bleeding, or unusual pain) promptly. Routine side effects are expected, but early management improves outcomes.
Conclusion
Radiation for endometrial cancer is highly individualized. Brachytherapy alone can be completed in a few outpatient sessions over 1–3 weeks; standard EBRT commonly runs 3–6 weeks; combined treatment typically totals 4–7 weeks. Advances in technology and hypofractionation can shorten courses for selected patients. A coordinated, multidisciplinary approach — with clear communication from surgeons like Dr. Lucas Minig and radiation oncologists — helps ensure the plan is both effective and manageable for your life and logistics, particularly when organizing care in Spain.