Worried about abnormal bleeding? Learn how estrogen Causes endometrial cancer, top risk factors (obesity, PCOS, HRT) and practical steps from Spanish specialist Dr. Lucas.
Introduction
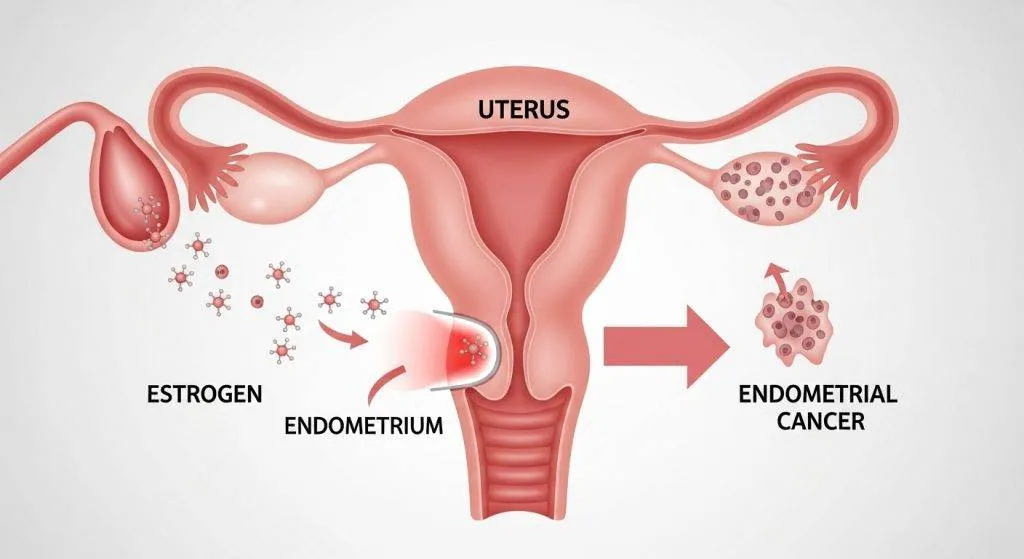
Estrogen plays a central role in the health of the uterus — it tells the endometrium (the uterine lining) when to grow and when to prepare for a possible pregnancy. When that signal becomes too frequent or isn’t balanced by progesterone, the risk of abnormal growth and cancer increases.
Below we unpack the biology, the step-by-step process from hormonal stimulation to cancer development, and practical points for patients in Spain — with notes on how doctors such as Dr. Lucas evaluate and manage risk.
Understanding Estrogen
Estrogen is a steroid hormone produced mainly by the ovaries in premenopausal women, and by peripheral tissues (like fat) after menopause. Think of it as a growth signal: in the uterus it tells cells to divide and prepare the lining for implantation.
Types of estrogen in the female body
There are three primary forms:
- Estradiol (E2) — the dominant form in reproductive years.
- Estrone (E1) — more common after menopause, produced in fat tissue.
- Estriol (E3) — prominent during pregnancy.
Each form has slightly different potency and tissue effects, and clinicians consider these differences when assessing risk.
Estrogen’s normal role in the menstrual cycle
During the follicular phase, estrogen levels rise and thicken the endometrium. After ovulation, progesterone from the corpus luteum tempers that growth, stabilizes the lining and readies it for implantation. If pregnancy doesn’t occur, hormone withdrawal leads to menstrual shedding — a healthy, cyclical turnover. When this balance is lost, problems can follow.
How Does Estrogen Cause Endometrial Cancer?
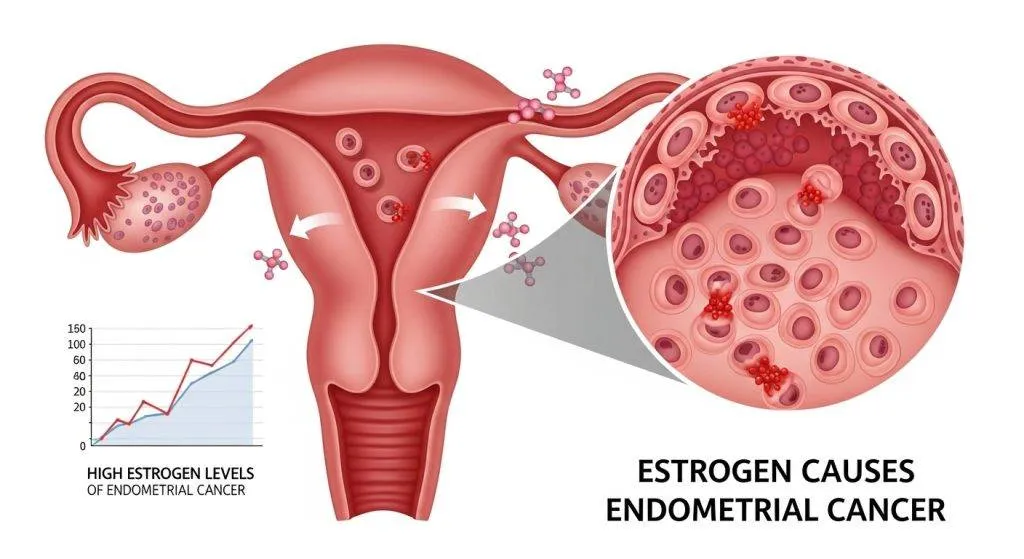
Estrogen itself does not “create” cancer instantly — rather, prolonged or excessive estrogenic stimulation increases cell division in the endometrium, which raises the chance of genetic mistakes and abnormal clones that can become malignant.
Clinicians describe this as a progression: persistent stimulation → thickening → precancerous change → potential cancer.
Continuous Stimulation of the Uterine Lining
When the endometrium is repeatedly signaled to grow without the normal counterbalance of progesterone, glands and cells proliferate excessively. More cell division means more opportunities for DNA errors; over time those errors can lead to cells that grow uncontrollably.
When Estrogen Acts Alone (Unopposed Estrogen)?
“Unopposed estrogen” is the clinical term for estrogen exposure without adequate progesterone protection. Causes include chronic anovulation (so no luteal-phase progesterone), estrogen-only hormone replacement therapy in women with a uterus, and peripheral estrogen production from adipose tissue. Each creates the biochemical environment that favors hyperplasia and cancer progression.
The Hormonal Balance That Protects the Uterus
When both hormones cycle normally, the lining grows, stabilizes and sheds predictably. If progesterone is insufficient or absent, the protective check is lost and the margin for error narrows.
Estrogen vs. Progesterone — The Natural Balance
Progesterone functions as a brake on estrogen’s accelerator: it reduces the proliferation signal, encourages orderly tissue maturation, and supports normal shedding. Doctors often focus on restoring or mimicking progesterone’s effect if they see prolonged estrogen exposure.
What Happens During a Normal Menstrual Cycle?
- Follicular phase: rising estrogen → endometrial proliferation.
- Ovulation: egg release.
- Luteal phase: progesterone rises → endometrium stabilizes and differentiates.
- If no pregnancy: hormones fall → menstruation.
This rhythm is the baseline of uterine health; disruptions to it are red flags in clinical assessment.
Step-by-Step: From Estrogen to Cancer Development
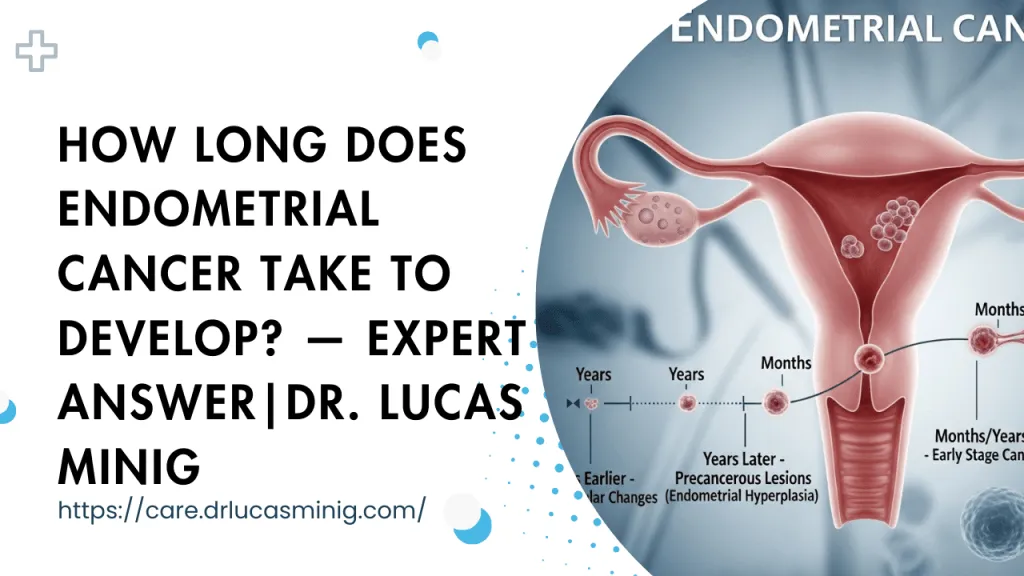
The progression from normal lining to cancer is usually gradual and detectable if surveillance is appropriate. Understanding each step helps patients and doctors intervene early.
Step 1 — Endometrial Thickening
Sustained estrogen exposure causes the uterine lining to thicken beyond normal cyclical variation. On ultrasound, this appears as an increased endometrial stripe; clinicians use thickness thresholds (age- and menopausal-status dependent) to decide on further tests.
Step 2 — Endometrial Hyperplasia
Hyperplasia means more glands and cells than normal. It can be:
- Simple hyperplasia — low risk, limited architectural change, often reversible.
- Atypical hyperplasia — cellular abnormalities (atypia) that carry a significantly higher risk of progression to carcinoma.
Doctors treat atypical hyperplasia more aggressively because it frequently represents a precursor lesion.
Step 3 — Cellular Changes and DNA Damage
With persistent proliferation, DNA repair mechanisms can be overwhelmed or fail. Mutations accumulate in genes that regulate growth, apoptosis and cell-cycle control. Over time, these molecular alterations can convert an atypical hyperplasia into invasive endometrial carcinoma.
When Hyperplasia Turns Into Cancer?
Not all hyperplasia becomes cancer, but atypical hyperplasia is the red line: many specialists recommend definitive treatment (medical progestin or surgery) depending on age, fertility desires and comorbidities. Early detection and treatment of atypia are crucial.
Who Is Most at Risk from Estrogen-Driven Endometrial Cancer?
Risk clusters around conditions that increase estrogen exposure or reduce progesterone. Identifying these situations allows targeted prevention and surveillance.
Obesity and Estrogen Production
Adipose tissue converts androgens to estrogen through aromatase activity; in people with obesity, this peripheral estrogen becomes a chronic source of unopposed stimulation — especially after menopause when ovarian production drops. That’s why weight management is a cornerstone of prevention.
PCOS and Irregular Ovulation
Polycystic ovary syndrome often causes infrequent ovulation, meaning prolonged periods without luteal progesterone. Over many years, that imbalance raises the risk of endometrial hyperplasia and cancer unless cycles are regulated medically.
Estrogen-Only Hormone Therapy
Women with an intact uterus who receive estrogen-only hormone therapy increase their endometrial cancer risk because progesterone’s protective effect is missing. For that reason, combined estrogen-progestin regimens are the standard when the uterus is preserved.
Early Periods, Late Menopause
Longer reproductive lifespan — early menarche or late menopause — increases the cumulative years of estrogen exposure. That lifetime exposure correlates with higher endometrial cancer risk, so clinicians include reproductive history in risk assessment.
Estrogen After Menopause — Why Risk Increases
After menopause, ovarian estrogen falls but peripheral conversion in fat continues; in women with obesity, this source can maintain estrogen levels that are relatively high for the postmenopausal state. Without cyclic progesterone to oppose it, the endometrium can be chronically stimulated, explaining the higher incidence of endometrial cancer in older age groups.
Protective Role of Progesterone
Progesterone opposes estrogen-driven proliferation by promoting differentiation and facilitating normal shedding. In clinical practice, progestin therapy (oral, injectable, intrauterine) is used both to treat hyperplasia and to reduce risk when estrogen exposure is necessary for other indications. Doctors tailor the approach—balancing symptom control, fertility goals and cancer prevention.
Symptoms That Should Never Be Ignored
The cardinal symptom to watch for is vaginal bleeding after menopause. Other red flags:
- New or irregular heavy periods (especially in perimenopausal women)
- Intermenstrual bleeding outside expected cycles
- Persistent pelvic pain or unexplained vaginal discharge (less common)
If you notice these signs, see a gynecologist promptly — earlier evaluation leads to earlier, less invasive treatment.
How Doctors in Spain Evaluate Estrogen? -Related Risk
Gynecologists in Spain follow pathways similar to international practice, with public and private options for diagnostics.
- Initial visit: history (bleeding pattern, HRT, family cancer syndromes like Lynch), physical exam.
- First-line test: transvaginal ultrasound to measure endometrial thickness.
- Definitive sampling: endometrial biopsy (office or under hysteroscopy) to get tissue diagnosis.
- Multidisciplinary review: pathology, radiology and oncology teams discuss confirmed cancers to plan surgery or adjuvant therapy.
Spanish clinicians also consider local resources: many public hospitals route through primary care referrals, while private clinics often offer faster direct access to imaging and specialist consultation.
Can You Lower Estrogen-Related Risk?
Yes — many strategies reduce exposure or mitigate its effects. A combined approach of lifestyle and medical measures yields the best results.
Weight Management
Losing weight reduces peripheral estrogen production, improves insulin sensitivity, and lowers inflammatory signals — all of which decrease endometrial stimulation. Even modest weight loss has measurable benefits.
Hormone Therapy Done Safely
If menopausal symptoms require HRT and the uterus is present, combined estrogen-progestin therapy is the safer option from an endometrial perspective. Discuss duration, regimen and monitoring with your physician to balance symptom relief and risk.
Birth Control Pills and Protection
Combined oral contraceptives (estrogen plus progestin) reduce endometrial cancer risk by providing regular progestin exposure and preventing unopposed estrogen effects. For many younger patients at risk, contraceptives are both effective birth control and risk-lowering therapy.
Modern Treatment if Cancer Develops
Treatment depends on stage and patient goals:
- Early-stage disease: surgery (hysterectomy with or without removal of ovaries and fallopian tubes) — often done minimally invasively.
- Fertility-sparing options: in carefully selected young patients with early, low-grade disease, high-dose progestin therapy and close surveillance may be considered.
- Advanced disease: surgery combined with radiotherapy, chemotherapy, or targeted treatments guided by molecular profiling.
Outcomes are generally favorable when cancer is detected early — another reason for prompt assessment of bleeding.
Meet Dr. Lucas (a clinical voice)
Dr. Lucas approaches each patient with a practical, evidence-based mindset: he blends clear patient education with careful diagnostic sequencing. In consultations, he explains hormone-driven mechanisms in plain language, outlines individualized prevention plans (weight, HRT counseling, surveillance), and coordinates rapid diagnostic pathways for symptomatic patients. Many patients appreciate his focus on balancing cancer prevention with quality-of-life and fertility considerations.
Dr. Lucas’s approach to diagnosis and treatment
Dr. Lucas focuses on prompt, evidence-based care with clear communication. His approach emphasizes:
- Rapid triage of abnormal bleeding.
- Use of transvaginal ultrasound followed by targeted biopsy or hysteroscopy when indicated.
- Personalized treatment plans — balancing oncologic safety with fertility preservation where desired.
Patients value his clear explanations, surgical skill in minimally invasive techniques, and coordinated care pathways.
How to arrange a consultation with Dr. Lucas in Spain?
Patients can schedule a teleconsult or in-person appointment through the clinic website or by contacting the clinic’s international patient coordinator. Bring prior imaging and reports to the first visit; this shortens time to diagnosis and treatment planning.
FAQs
Can endometrial cancer be caused by normal estrogen use?
Normal cyclical estrogen (with ovulation and luteal progesterone) is not a cause; the risk increases when estrogen exposure is chronic and unopposed. Always discuss HRT plans with your doctor.
If I have PCOS, does that mean I will get endometrial cancer?
No — PCOS increases risk but doesn’t guarantee cancer. Managing cycles (e.g., with progestin or combined oral contraceptives) and regular follow-up significantly reduce risk.
Is weight loss really effective in lowering risk?
Yes. Reducing body fat lowers peripheral estrogen production and improves metabolic health, which together reduce endometrial stimulation.
What should I do if I notice postmenopausal bleeding in Spain?
See a gynecologist promptly or contact your GP for urgent referral. Early ultrasound and biopsy will clarify the cause; most early-stage conditions are very treatable.
Can fertility be preserved if hyperplasia or early cancer is found?
In selected patients with atypical hyperplasia or very early, low-grade cancer, fertility-sparing options (high-dose progestins, hysteroscopic resection) may be considered under specialist care, with close follow-up and expert counseling.
Conclusion
Estrogen is vital but powerful: when its proliferative signal to the endometrium is prolonged or unopposed, the risk of hyperplasia and eventual endometrial cancer rises. The good news is that many risk factors are modifiable, and early evaluation of abnormal bleeding leads to prompt, effective treatment. For people in Spain, local specialists — including clinicians like Dr. Lucas — offer structured assessment and tailored plans that combine prevention, safe hormone therapy, and timely treatment when needed.