Learn how tumor diameter affects staging, lymph-node risk and treatment choices. Expert, Spain-based guidance from Dr. Lucas Minig in Valencia — what to ask your doctor.
Introduction
Tumor size is one of those pieces of information that patients notice on a radiology or pathology report and immediately treat like a verdict. “How big is it?” feels like the most basic question — and it matters. But in endometrial cancer, size is important yet not decisive: it helps doctors estimate risk, plan surgery, and guide conversations about fertility and adjuvant therapy, but it must be interpreted together with grade, histology, imaging and other findings. Below I explain exactly what clinicians mean by “tumor size,” how it’s measured, why the method matters, and how size fits into staging, prognosis and treatment — including a practical Spain-focused perspective from Dr. Lucas Minig’s clinic in Valencia.
Understanding Tumor Size
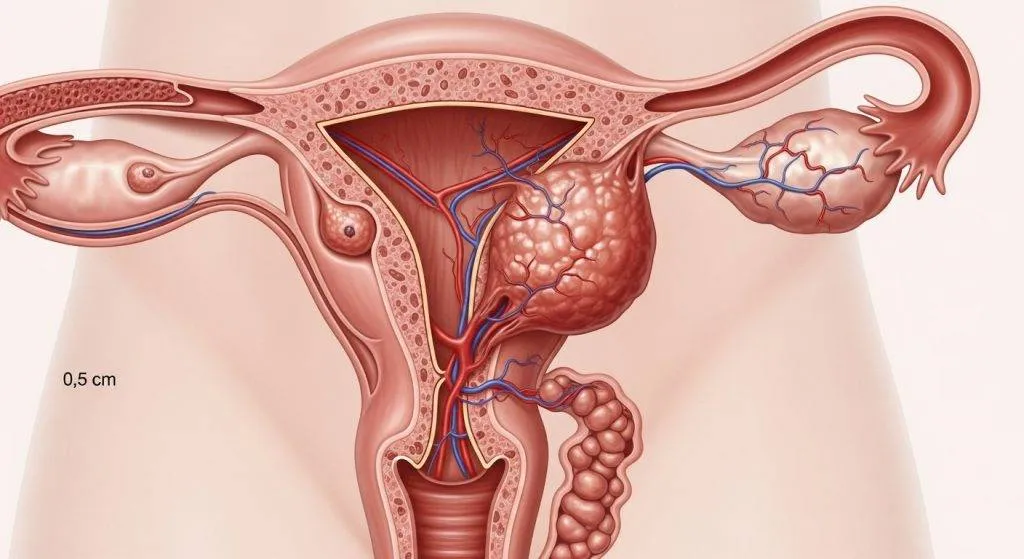
When clinicians talk about tumor size in endometrial cancer they usually mean the maximum diameter of the visible tumor (the longest single measurement) — either estimated on imaging (pre-operative) or measured directly on the surgical specimen by the pathologist. That single number is a convenient shorthand, but remember: tumors are three-dimensional, sometimes multifocal, and may spread along the lining rather than form a neat ball.
How tumor size is measured (imaging vs surgery)?
- Imaging (pre-op): Transvaginal ultrasound (TVUS) and MRI are the common tools. TVUS is quick and accessible; MRI gives better soft-tissue contrast and a more accurate estimate of diameter and depth of myometrial invasion.
- Surgical/pathology measurement (post-op): Once the uterus is removed, the pathologist measures the tumor directly on the specimen—this is the “gold standard” for definitive diameter, but it can differ from imaging for several reasons.
Why measurement method matters?
- Tissue handling: Formalin fixation and slicing can cause shrinkage or fragmentation, so pathology size may be slightly different than in vivo measurements.
- Multifocal or diffuse tumors: MRI may underestimate tumor extent when disease spreads as a thin layer along the endometrium; conversely, small satellite lesions may be missed on imaging but found by pathology.
- Operator and technique variability: Ultrasound is operator-dependent; MRI interpretation depends on sequence quality and radiologist expertise. These differences influence clinical decisions — so clinicians always interpret “size” with the measurement method in mind.
Does Tumor Size Matter in Endometrial Cancer?
Yes — tumor size matters — but it’s one factor among several. Larger tumors are statistically associated with deeper myometrial invasion, higher rates of lymphovascular space invasion (LVSI) and greater risk of lymph node metastasis; however, tumor size alone does not determine stage or prognosis without considering grade, histology and node status. Large size raises suspicion and often triggers more extensive staging and treatment workup.
Why doctors look beyond size?
Histologic grade (how abnormal the cells look), histologic subtype (endometrioid vs serous/clear cell), presence of LVSI, and depth of myometrial invasion typically predict behavior as much or more than size. A small high-grade serous tumor can be more aggressive than a larger, low-grade endometrioid tumor. That’s why multidisciplinary teams integrate multiple variables into a treatment plan rather than relying on diameter alone.
Why Tumor Size Can Influence Cancer Behavior?
Tumor size is tied to biological behavior because a larger mass often reflects more time for the cancer to invade adjacent tissue and spread.
Larger tumors and deeper invasion
Larger diameter frequently goes hand-in-hand with deeper myometrial invasion—a key determinant of stage and future risk. Deep myometrial invasion is a major reason oncologists worry about nodal spread and consider adjuvant therapy.
Tumor size and lymphovascular space invasion (LVSI)
Studies show that tumours of greater size have higher rates of LVSI, which indicates that cancer cells can travel through lymphatic/blood channels—this marker predicts a higher chance of recurrence and influences recommendations for radiotherapy or chemotherapy.
Tumor size and lymph node spread
Several recent analyses link increasing tumour diameter with rising lymph node positivity rates. For example, a 2024 study reported essentially zero node positivity below a certain diameter threshold and measurable increases above it — a finding that affects decisions about sentinel node mapping vs full nodal dissection.
Tumor Size and Cancer Staging
Size is not the same as stage, but it plays an important background role in how teams interpret staging data and choose management.
FIGO staging explained simply
FIGO staging classifies uterine cancer by how far it has spread: whether it is confined to the uterus, has invaded the cervix or myometrium deeply, or has moved to lymph nodes or distant organs. The staging number reflects spread, not measurement in centimetres.
Why tumor size is not directly in the stage number?
Because staging focuses on extent rather than volume, FIGO does not include maximum tumour diameter as a numeric staging criterion. A small tumour with nodal metastasis can be higher stage, while a larger tumour confined to the endometrium can remain stage I.
How size still influences staging decisions?
Although not part of the stage number, size informs whether a surgeon pursues more thorough nodal assessment or whether a case should be treated more aggressively after final pathology—so it indirectly shapes the management that follows staging.
Research Findings on Tumor Size and Outcomes
Research consistently links increasing size with rising recurrence and, in some series, worse survival — but nuance matters.
Recurrence risk
Larger tumours are associated with higher recurrence rates in many cohorts, particularly when combined with LVSI, high grade, or non-endometrioid histology. Some researchers recommend using thresholds (e.g., 2–4 cm) to flag higher recurrence risk.
Survival rates and tumor diameter
Population studies going back decades show survival declines as diameter increases, but contemporary data emphasize that molecular profile and histology often account for much of this effect—size tends to be a proxy for other aggressive features in many analyses.

Small Tumors: Are They Always Low Risk?
No. Small tumor diameter markedly lowers the probability of adverse features, especially when the tumor is low-grade and imaging shows minimal invasion — but exceptions occur. Small high-grade tumors or non-endometrioid histologies (serous/clear cell) can behave aggressively. So, “small” reduces risk but does not eliminate it.
Large Tumors: Does Bigger Always Mean Worse?
“Bigger” increases the odds of aggressive features, but not always. A large, well-differentiated endometrioid tumor without LVSI or node involvement can still have a favorable outcome after appropriate surgery. Conversely, a modestly sized aggressive subtype may fare worse. Clinical context is everything.
How Tumor Size Affects Treatment Decisions in Spain?
Spanish clinicians use tumor size as a routine datapoint in multidisciplinary planning—integrating it with local protocols and European guidelines. In practice, size shapes surgical technique, nodal assessment and fertility options.
Surgical planning
Surgeons use MRI size estimates to decide if minimally invasive surgery is feasible and whether intraoperative frozen section or sentinel node mapping is planned. At private and public centres in Spain, having a clear MRI measurement before surgery is a standard part of planning.
Lymph node assessment
A larger measured tumor pushes teams to have a lower threshold for sentinel lymph node mapping or formal lymphadenectomy because of the correlation with node positivity. Decisions are individualized using size plus grade and LVSI status.
Fertility-sparing treatment considerations
For women considering fertility preservation, tumor size matters: small, low-grade, superficial tumours are the usual candidates for conservative hormonal treatment, whereas larger tumours usually disqualify this route. Multidisciplinary evaluation and accurate imaging are essential.
When tumor size matters most?
Size is most useful when a case sits on the borderline between conservative and aggressive management. It’s also decisive when planning the extent of surgery.
Low-grade, presumed early disease
In low-grade endometrioid tumours with small MRI size and superficial invasion, many clinicians opt for minimally invasive hysterectomy with sentinel node mapping and often no adjuvant therapy.
High-grade or non-endometrioid histology
When histology is aggressive (serous, clear cell) or the tumour is high-grade, molecular and histologic features overshadow size. Even small aggressive tumours may need comprehensive staging and adjuvant therapy.
What Pathologists Look for Besides Size?
Pathologists are detectives. Size is recorded, but they also report several characteristics that often matter more for prognosis and treatment.
Tumor grade
Grade (how abnormal the cancer cells look) predicts behavior—high grade predicts worse outcomes and usually triggers more aggressive treatment decisions.
Histological subtype
Non-endometrioid types (serous, clear cell, carcinosarcoma) have higher recurrence risk even at small sizes.
Depth of myometrial invasion
This is one of the clearest stage-and-prognosis determinants—pathologists quantify invasion and this measurement strongly affects post-op recommendations.

Dr. Lucas Minig — what he recommends (clinic perspective)
At Dr. Lucas Minig’s Valencia clinic, tumour size is treated as an important clue but always within a full diagnostic picture. Dr. Minig emphasizes fast, precise work-ups and individualized plans.
How Dr. Lucas interprets size with MRI and pathology?
Dr. Minig prioritises high-quality MRI before surgery and rapid pathology review after surgery so that size can be combined with grade, LVSI and molecular testing to guide treatment—he and his team aim to complete imaging, biopsy and staging assessments within days for prompt decisions.
What Dr. Lucas recommends for patients in Spain? (Valencia clinic)
In Valencia, Dr. Minig offers minimally invasive and robotic surgery, sentinel node techniques, rapid second opinions and personalised follow-up. He advises patients to bring MRI images and pathology reports to consultations so size and other factors are interpreted together, and he will explain whether size changes the recommended surgical plan or adjuvant therapy.
Conclusion
Tumor size in endometrial cancer is a useful and actionable marker: larger diameter correlates with deeper invasion, LVSI and higher nodal risk, and it influences surgical planning and risk stratification. But size is never an isolated verdict — histology, grade, imaging findings and multidisciplinary judgment determine the final stage and treatment. In Spain, clinicians routinely incorporate size (commonly using 2 cm as a pragmatic cutoff in many algorithms) into preoperative planning, and expert teams — such as Dr. Lucas Minig’s clinic in Valencia — use MRI, pathology and patient goals to individualize care.
FAQs
Is tumor size the same as cancer stage?
No. Stage describes how far the cancer has spread; size is a measurement that helps predict risk and guide management.
Can MRI measurements replace pathology for tumour size?
MRI is excellent for planning and estimating size, but the final pathology measurement after surgery is the definitive value.
If my tumor is small, do I always avoid lymph node surgery?
Not always—small tumors frequently have low nodal risk, but decisions depend on grade, LVSI and molecular features; sentinel node mapping is often used for precise assessment.
Does a tumour >4 cm mean a worse prognosis?
Larger tumours have a higher association with adverse features and recurrence, but prognosis depends on multiple factors—size alone does not determine outcome.
How can Dr. Lucas Minig help patients concerned about tumor size?
Dr. Minig’s Valencia clinic offers rapid imaging, specialist pathology review, minimally invasive surgery and personalised care plans—he advises patients to seek a multidisciplinary opinion and bring complete imaging and pathology records.