Discover when a hysterectomy can cure endometrial cancer, treatment options, minimally invasive surgery and expert care in Spain with Dr. Lucas Minig.
Introduction
A common, urgent question for patients diagnosed with uterine cancer is: does hysterectomy cure endometrial cancer? The short, accurate answer is: often — particularly for early, uterine-confined disease — but not always. A hysterectomy is the fundamental first-line treatment for most cases of endometrial cancer because it removes the organ where the cancer began and provides essential information that determines whether additional (adjuvant) treatment is required. This article explains what a hysterectomy involves, when it can be curative, when more treatment is needed, and what patients in Spain — and elsewhere — should expect.
What Is a Hysterectomy?
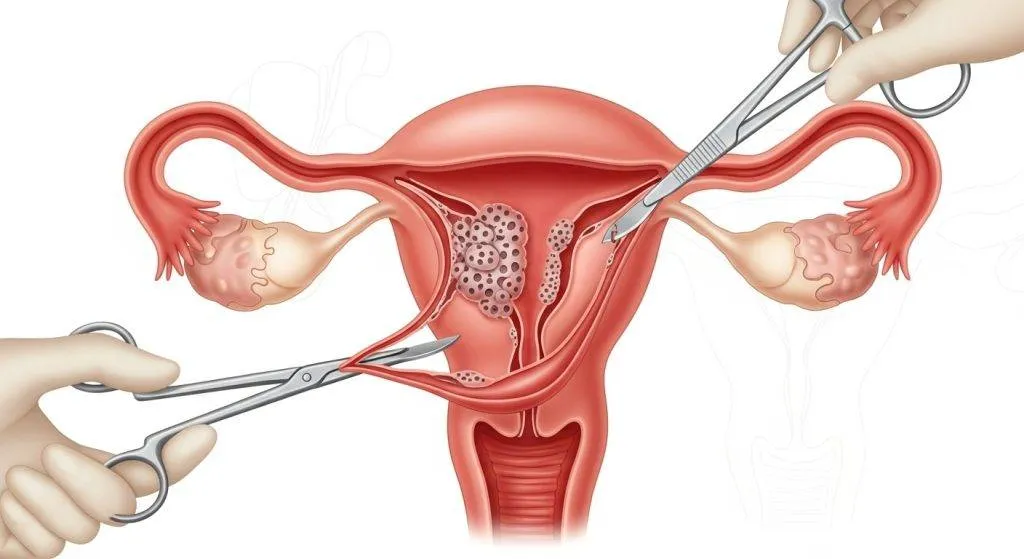
A hysterectomy is a surgical procedure that removes the uterus. For cancer treatment, the operation is tailored to remove disease safely and to stage the cancer accurately so clinicians can recommend further therapy if necessary. The exact type of hysterectomy and the extent of surgery depend on the tumour’s stage, grade, patient age, and fertility wishes.
At specialised centres in Spain — including clinics led by surgeons such as Dr. Lucas Minig — hysterectomy for cancer is performed with particular attention to oncologic safety, minimally invasive technique, and rapid recovery.
Types of Hysterectomy Used in Endometrial Cancer
- Total Hysterectomy: A total hysterectomy removes the uterus and the cervix. This is the most commonly performed hysterectomy for endometrial cancer when the disease appears confined to the uterine cavity.
- Radical Hysterectomy: A radical hysterectomy removes the uterus, cervix, upper vagina, and the surrounding parametrial tissue. It is usually reserved for cancers that directly involve the cervix or when a wider margin is needed for disease control.
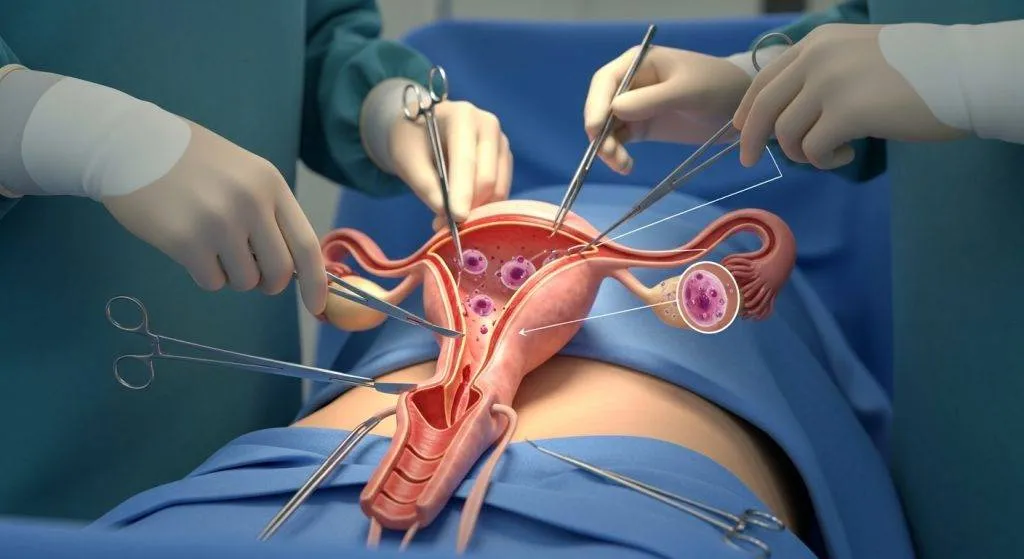
- Hysterectomy With Bilateral Salpingo-Oophorectomy: Most patients with endometrial cancer will have a hysterectomy with bilateral salpingo-oophorectomy (BSO) — removal of both ovaries and fallopian tubes — at the same operation. Removing the ovaries eliminates a potential source of hormone production and reduces the risk of occult ovarian involvement in older patients.
What surgeons usually remove for endometrial cancer (BSO, nodes)?
Standard oncologic surgery for endometrial cancer frequently includes:
- Total hysterectomy + bilateral salpingo-oophorectomy (BSO)
- Lymph node assessment via sentinel lymph node mapping or selective lymphadenectomy, depending on clinical factors
- Occasionally peritoneal sampling or omentectomy in certain aggressive histologic subtypes
These steps both treat and stage the disease—critical to deciding whether the patient needs additional therapies like radiation or chemotherapy.
Does a Hysterectomy Cure Endometrial Cancer?
A hysterectomy can cure endometrial cancer when the disease is confined to the uterus and has favourable biological features (low grade, shallow myometrial invasion). For many patients with stage I, low-grade endometrioid tumours, surgical removal of the uterus and adnexa is sufficient and results in high long-term disease-free survival.
However, if pathology shows high-risk features, deep invasion, lymphovascular spread, nodal involvement, or distant metastases, a hysterectomy alone is unlikely to be curative and is usually followed by adjuvant therapies to control microscopic or overt spread.
Why Hysterectomy Is the Cornerstone of Treatment?
Surgery plays two indispensable roles:
- Therapeutic — it removes the primary tumour and the organ that hosts it.
- Diagnostic/staging — the pathology report (tumour grade, depth of invasion, lymph node status, molecular markers) determines prognosis and the need for radiation, chemotherapy, or hormone therapy.
Because of these dual purposes, hysterectomy is the foundation on which subsequent treatment decisions are built.
When a Hysterectomy Can Be Curative?
When endometrial cancer is limited to the uterus and demonstrates low-risk features, surgery alone often provides a cure. Below are the typical clinical situations where that outcome is most likely.
Early stage (stage I) disease and low-grade tumours
Stage I disease — where the tumour is confined to the endometrium or invades only the inner portion of the myometrium — and low-grade (well-differentiated) histology are the best scenarios for surgical cure. In these cases, a hysterectomy with BSO and appropriate node assessment frequently removes all cancerous tissue.
Expected outcomes and survival statistics
Outcomes vary by tumour biology, but many patients with stage I, low-grade endometrioid cancers achieve excellent long-term survival after surgery alone. At specialised practices in Spain, where minimally invasive techniques and modern staging are routine, these favourable results are commonly reported. Patients should discuss their individualized prognosis with their treating gynecologic oncologist.
When Hysterectomy Alone Is Not Enough?
Not all endometrial cancers are cured by surgery alone. Certain features increase the likelihood that additional therapy will be required.
High-risk pathology and deeper invasion
High tumour grade, deep myometrial invasion, lymphovascular space invasion, and aggressive histologic subtypes (such as serous or clear cell) are associated with higher recurrence risk. When these features appear in pathology, adjuvant radiation and/or chemotherapy is commonly recommended to reduce recurrence risk.
Lymph node involvement and metastatic disease
If cancer is found in pelvic or para-aortic lymph nodes, or if imaging or intraoperative findings suggest spread beyond the pelvis, a hysterectomy remains an important component of treatment but is not considered curative on its own. Systemic therapy (chemotherapy, and increasingly targeted or immunotherapeutic agents) and radiation become central to treatment in these scenarios.
Minimally Invasive Surgery: Benefits & Use in Spain
Minimally invasive approaches (laparoscopic and robotic surgery) are standard for many early endometrial cancer cases. In Spain, numerous tertiary centres and experienced surgeons routinely offer these techniques, which reduce the surgical footprint while preserving oncologic outcomes.
Laparoscopic and robotic approaches
Laparoscopic and robotic hysterectomies allow surgeons to perform precise dissections through small incisions. These approaches facilitate sentinel node mapping and BSO while minimizing blood loss and surgical trauma.
Faster recovery, fewer complications
Key advantages include shorter hospital stays, reduced postoperative pain, lower infection risk, and faster return to normal activities—factors that matter to patients who want to resume life quickly while maintaining optimal cancer control.
The Role of Lymph Node Assessment and Sentinel Node Mapping
Lymph node status is a major prognostic indicator. Sentinel lymph node (SLN) mapping identifies the first nodes that drain the uterus; if these nodes are clear, the likelihood of broader nodal spread is low. SLN mapping reduces the need for comprehensive lymphadenectomy and its associated complications (lymphedema, nerve injury), and has become a preferred strategy in many European centres.
Surgeons like Dr. Lucas integrate SLN mapping into routine staging to balance diagnostic precision with patient safety.
What Other Treatments May Be Needed After a Hysterectomy?
After surgery, the pathology report guides additional therapy.
Radiation Therapy
Used to reduce local recurrence risk, radiation options include external beam radiotherapy (EBRT) and vaginal brachytherapy. Choice depends on risk factors identified at surgery.
Chemotherapy
Systemic chemotherapy is standard for advanced-stage disease and for some high-risk histologies. Combinations such as carboplatin and paclitaxel are commonly used.
Hormonal and Targeted Therapies
Hormonal therapy (progestins) can be effective in hormone-receptor–positive tumours and is sometimes used for low-grade disease or as a fertility-sparing alternative. Targeted therapies and immunotherapies are options for selected molecular subtypes in advanced disease.

Life After a Hysterectomy for Endometrial Cancer
Understanding recovery and long-term effects helps patients prepare mentally and physically for life after surgery.
Recovery Timeline
- Immediate postoperative (0–2 weeks): pain control, wound care, gradual mobilization.
- Subacute (2–6 weeks): resuming light activities; most minimally invasive patients return to routine in 4–6 weeks.
- Long term (>6 weeks): recovery of full activity depends on adjuvant therapy and individual factors.
Hormonal Changes and Menopause
If ovaries are removed, women experience surgical menopause: hot flashes, vaginal dryness, mood changes, and possible bone loss. Hormone replacement therapy is a nuanced decision in cancer patients and must be discussed case-by-case with the oncology team.
Emotional and Psychological Impact
Even when the surgery is technically successful, patients may face grief over fertility loss, body image changes, and anxiety about recurrence. Psychological support, counselling, and peer support groups are important components of holistic care.
Can Endometrial Cancer Come Back After a Hysterectomy?
Recurrence is possible, although risk varies widely according to initial stage and tumour biology. Early detection and surveillance are key components of survivorship.
Understanding Recurrence Risk
Recurrence is uncommon for low-risk, early-stage disease but increases with high-risk features. Recurrences may be local (vaginal cuff), regional (pelvis, nodes), or distant (lungs, liver). Tumour biology strongly influences recurrence patterns.
Importance of Follow-Up Care
Regular follow-up visits — pelvic exams, symptom review, targeted imaging when indicated — allow early detection and treatment of recurrence. In Spain, multidisciplinary follow-up pathways ensure coordinated care between surgeons, medical oncologists, and radiation oncologists.
Choosing the Right Doctor like Dr. Lucas for Endometrial Cancer Treatment in Spain
Selecting a specialised gynecologic oncologist significantly impacts outcomes. Look for surgeons with cancer-specific expertise, high procedural volumes, and access to a multidisciplinary team.
Why Specialized Gynecologic Oncologists Matter
Gynecologic oncologists have specialized training in cancer surgery and staging. Outcomes are better when operated on by surgeons and teams experienced with oncologic principles and minimally invasive techniques.
Personalized Cancer Care in Spain
Spanish centres with dedicated gynecologic oncology programs emphasize individualized plans—tailoring the extent of surgery, lymph node strategy, and adjuvant therapy to the patient’s tumour biology and personal preferences. Specialists such as Dr. Lucas Minig are examples of clinicians who integrate advanced surgical technique with a patient-centred approach.

Fertility Considerations and Alternatives
When fertility preservation is a priority, alternatives to immediate hysterectomy may be considered in very select early cases; however, such approaches require careful selection and intensive follow-up.
Can fertility be preserved in any cases?
In highly selected young patients with very early, low-grade endometrial cancer (and strong desire to preserve fertility), conservative management with high-dose progestins or hysteroscopic resection plus hormonal therapy may be considered under strict surveillance. This approach carries risks and requires informed, close follow-up.
Why hysterectomy ends pregnancy potential
A hysterectomy removes the uterus, so natural pregnancy is no longer possible afterward. For patients who wish to preserve fertility, early discussion with their care team, including reproductive specialists, is essential.
How Dr. Lucas Minig and Similar Specialists Approach Surgery in Spain?
Specialist surgeons in Spain prioritize:
- Accurate preoperative staging (imaging, biopsy)
- Minimally invasive hysterectomy with BSO when appropriate
- Sentinel node mapping to minimize morbidity while optimizing staging
- Multidisciplinary planning for adjuvant therapy when needed
They also emphasize patient education, recovery planning, and psychosocial support.
FAQs
Does a hysterectomy always mean I will not need radiation or chemo?
No. Whether radiation or chemotherapy is needed depends on the final pathology report (stage, grade, lymph node status). Many early, low-risk cases need only surgery; higher-risk cases will receive adjuvant therapy.
If my ovaries are removed, will I need hormone replacement?
Surgical removal of ovaries causes menopause. Hormone replacement therapy may be considered depending on your cancer type and risk; this requires a careful, case-by-case discussion with your oncologist.
How long is recovery after a minimally invasive hysterectomy?
Most patients return to light activity within 1–2 weeks and to normal activities in about 4–6 weeks, although recovery varies by individual and whether adjuvant therapy is required.
Is sentinel lymph node mapping as accurate as full node removal?
Sentinel lymph node mapping is highly accurate for staging in appropriately selected patients and reduces the risk of complications associated with complete lymphadenectomy.
Where should I go in Spain for endometrial cancer surgery?
Seek centres with dedicated gynecologic oncology teams, high surgical volumes, and expertise in minimally invasive and sentinel node techniques. Specialists such as Dr. Lucas Minig — and similar experienced surgeons in tertiary Spanish centres — offer multidisciplinary, personalized care.
Conclusion
A hysterectomy is the primary and often curative treatment for many women with early-stage endometrial cancer. Its curative potential depends on tumour stage, grade, and biology; when risk factors exist, additional therapies are essential to improve outcomes. Choosing an experienced gynecologic oncologist and a multidisciplinary centre — such as those in Spain where specialists like Dr. Lucas Minig practice — ensures the most appropriate balance between effective cancer control and quality of life.