Can you get pregnant with endometrial cancer? Learn when pregnancy is possible, fertility-sparing treatments, IVF and egg-freezing options — expert care from Spanish specialists.
Introduction
Being told you have endometrial (uterine) cancer triggers immediate questions about survival — and, for many women, an equally urgent question about children. Fertility concerns are not secondary; they shape treatment choices, emotional responses, and the timeline for care.
This article explains, clearly and compassionately, how endometrial cancer and pregnancy interact, what treatment-options preserve fertility, and how care teams in Spain — including doctors like Dr. Lucas Minig — manage these complex decisions.
Why this question matters
Fertility is time-sensitive and deeply personal. When cancer occurs at a reproductive age, the stakes include both oncologic safety and future parenthood. That’s why modern care emphasizes timely counseling and coordinated onco-fertility planning.
Understanding Endometrial Cancer
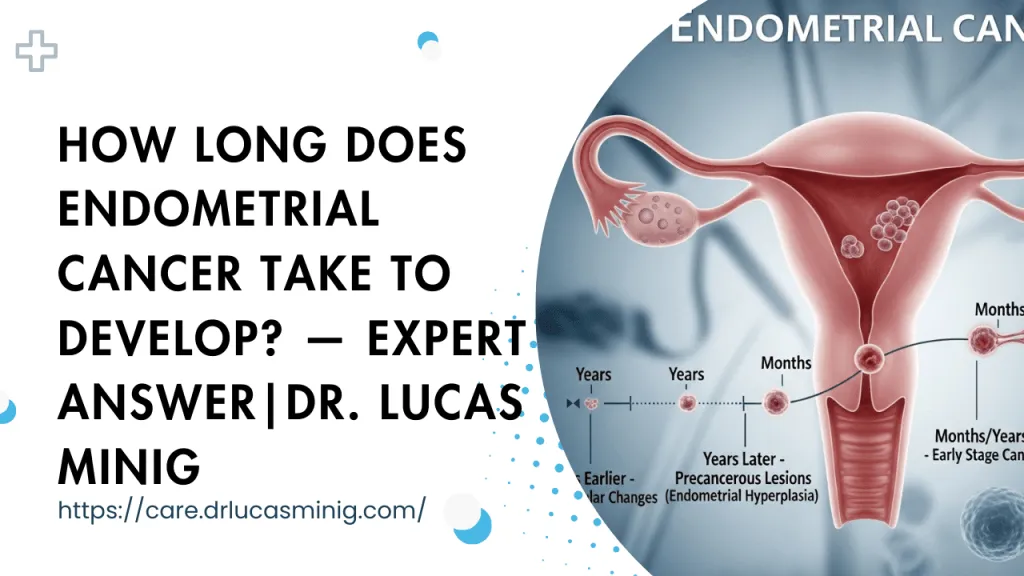
Endometrial cancer starts in the lining of the uterus (the endometrium). Because the lining is the very tissue that must be healthy for an embryo to implant, disease has direct implications for pregnancy.
Understanding the biology helps explain why fertility-preserving approaches are limited to specific, low-risk situations.
Why does this cancer directly affect pregnancy?
Imagine trying to plant a seed in burned soil: the soil may not support growth even if the seed is otherwise healthy. Similarly, when the endometrium is diseased or scarred by cancer, implantation becomes difficult or impossible. In addition, some tumors produce hormonal changes that interfere with ovulation and the wider reproductive environment.
Can You Get Pregnant With Endometrial Cancer?
It depends on the stage and grade of the tumor, the presence of spread beyond the lining, the patient’s age and ovarian reserve, and the available treatment pathway. For selected patients with early, low-grade tumors, fertility-sparing options exist. For others, standard curative treatment removes the uterus and with it the ability to carry a pregnancy.
The honest medical reality
The standard curative treatment for most endometrial cancers is hysterectomy (removal of the uterus), often with removal of fallopian tubes and sometimes ovaries — which eliminates the possibility of carrying a pregnancy. For selected early cases, however, conservative treatment can allow pregnancy attempts.
Why the answer is not always “no”
Medicine has moved beyond a single “one-size-fits-all” response. In well-selected cases—typically young patients with FIGO stage IA, grade 1 endometrioid carcinoma confined to the endometrium—doctors may offer conservative management that aims to control disease while preserving the uterus. This gives a window for conception, often assisted by reproductive technologies.
How Endometrial Cancer Affects Fertility
Effects combine mechanical (tissue damage), hormonal (imbalance), and procedural (surgery) factors.
Implantation problems
The endometrium must be receptive for an embryo to implant. Cancer disturbs that receptivity by altering the tissue architecture, inflaming the lining, or creating local environments unfavorable to embryo attachment. Even after treatment, scarring or regeneration abnormalities can cause ongoing implantation difficulty.
Hormonal imbalance and ovulation issues
Endometrial cancer is often linked to prolonged estrogen exposure relative to progesterone (so-called estrogen dominance). Conditions associated with hormonal imbalance—such as PCOS or obesity—both increase endometrial cancer risk and interfere with regular ovulation. So infertility may be present before cancer is treated.
Is Pregnancy Possible Before Treatment?
In rare cases pregnancy is ongoing at diagnosis or can occur briefly before treatment begins. These situations are medically complex and require immediate multidisciplinary input.
Pregnancy concurrent with active endometrial malignancy is unusual and usually carries heightened risk for both mother and pregnancy.
Rare but documented cases
There are documented cases of women who conceived before diagnosis or who were unknowingly pregnant at diagnosis. These situations are uncommon and medically complex. Pregnancies discovered alongside cancer require individualized risk assessment because cancer management and fetal safety must both be weighed.
Why it’s medically risky
Pregnancy changes hormone levels (notably increasing estrogen and progesterone) and may make decision-making and treatment timing more complicated. Delaying oncologic treatment for the sake of pregnancy risks progression; proceeding with cancer treatment may jeopardize the pregnancy. These cases require multidisciplinary care—obstetrics, oncology, and reproductive medicine working in close coordination.
Standard Treatment and Its Impact on Pregnancy
The standard of care for most endometrial cancers is surgery; this is highly effective for oncologic control but usually ends the ability to carry a pregnancy.
Knowing the implications of each treatment choice is essential when fertility is a concern.
Hysterectomy and fertility loss
The standard curative treatment for most endometrial cancers is total hysterectomy (removal of the uterus), often with bilateral salpingo-oophorectomy (removal of both ovaries and fallopian tubes) depending on patient age and tumor characteristics. Once the uterus is removed, carrying a pregnancy naturally is no longer possible.
Ovarian removal and early menopause
If ovaries are removed, a woman enters surgical menopause: natural hormone production stops and eggs are no longer available. Before ovary removal, many clinics recommend egg or embryo freezing if future biological parenthood is desired.
Fertility-Sparing Treatment: A Hopeful Option
For certain low-risk tumors, clinicians may offer treatments that manage the cancer while preserving the uterus — at least temporarily. This is a carefully monitored compromise aimed at balancing fertility desires with cancer control.
Fertility-sparing treatment is not experimental; it is guided by recent evidence and European consensus statements for appropriate candidates.
What fertility-sparing treatment means
“Fertility-sparing” describes medical strategies that aim to treat or control the cancer while preserving the uterus so the patient can attempt pregnancy. These are not suitable for all cancers and require stringent selection and close follow-up.
Hormonal therapy explained (progestins & IUDs)
Progestin therapy counteracts unopposed estrogen and can induce regression in selected low-grade endometrial cancers and in complex atypical hyperplasia. Options include:
- High-dose oral progestins (e.g., medroxyprogesterone acetate or megestrol acetate).
- Levonorgestrel-releasing intrauterine device (IUD), which delivers progestin directly to the endometrium.
Treatment typically lasts several months with repeated endometrial sampling to confirm response. If the tumor regresses, the patient and her doctors may plan a timed attempt at conception (frequently with IVF to shorten time-to-pregnancy).
Who Is Eligible for Fertility-Sparing Treatment?
Eligibility is strict because safety is the top priority. Only a subset of patients can consider conservative management.
Careful selection ensures the best chance of both cancer control and later pregnancy.
Cancer stage and grade requirements
Eligibility generally requires:
- Tumor confined to the endometrium (no myometrial invasion).
- Low histologic grade (usually grade 1 endometrioid carcinoma).
- No evidence of metastatic disease on imaging.
Age and reproductive goals
Younger age and a clear, realistic desire for pregnancy are factors in favor of pursuing conservative therapy. Patients must be willing to accept oncologic trade-offs and to proceed quickly with conception once cancer is under control.
Medical criteria doctors use
Before offering fertility-sparing treatment, clinicians perform:
- MRI to assess depth of invasion.
- Hysteroscopic or pipelle endometrial biopsy for pathology.
- Hormone receptor testing and thorough clinical staging.
Decisions are made in multidisciplinary tumor boards with gynecologic oncologists, pathologists and reproductive specialists.
How Doctors (Like Dr. Lucas Minig) in Spain Manage Fertility-Sparing Care
In Spain, specialized teams coordinate oncology and reproductive care to offer timely, safe fertility options. Clinicians such as Dr. Lucas Minig work within multidisciplinary groups to align cancer treatment and fertility preservation.
Patients referred early to such teams gain access to expedited egg/embryo preservation, structured progestin protocols, and joint decision-making.
Multidisciplinary cancer teams
Centers in Spain that specialize in onco-fertility adopt a team approach: gynecologic oncologist, reproductive endocrinologist, radiologist and often a psycho-oncology counselor. This coordinated care speeds decision-making and allows rapid access to egg/embryo preservation.
Role of gynecologic oncologists and fertility specialists
Gynecologic oncologists manage the cancer treatment plan and surveillance; fertility specialists focus on ovarian stimulation, egg/embryo cryopreservation and the timing of assisted reproduction. Clinics led by experienced surgeons—such as those modeled by Dr. Lucas Minig’s practice—prioritize minimally invasive assessment and fast referral to fertility services when fertility preservation is desired.
Pregnancy Success Rates After Conservative Treatment
Outcomes vary widely depending on selection, age, and use of assisted reproduction. Conservative therapy can lead to remission and pregnancy in many cases, particularly when
IVF is used to shorten the time to conception.
Natural conception vs IVF
- Natural conception is possible after remission but may be slower and less reliable due to underlying ovulatory or endometrial issues.
- IVF is often recommended to increase pregnancy probability quickly and to reduce the duration the endometrium is exposed to fluctuating hormones.
What studies and real cases show
Outcomes vary by center and patient selection. Published reviews report pregnancy rates that range widely—reflecting differences in treatment protocols, patient age, and use of assisted reproduction. The key takeaway: with careful selection and a proactive reproductive plan, a meaningful proportion of women can achieve pregnancy after conservative treatment, especially when IVF is used.
Risks of Delaying Surgery to Get Pregnant
Choosing conservative therapy is a trade-off: the goal is pregnancy without compromising cancer outcomes.
This makes rigorous follow-up and patient understanding critical.
Cancer recurrence risk
Delaying definitive surgery to attempt pregnancy carries a measurable recurrence risk. Patients and their doctors must weigh the oncologic risk against fertility desires. If disease fails to respond or recurs, prompt definitive surgery is recommended.
Importance of strict monitoring
Fertility-sparing care requires strict follow-up: routine endometrial sampling (every 3–6 months initially), periodic imaging, and a clear plan for definitive hysterectomy after childbearing is complete or if disease persists. Close monitoring is non-negotiable.
IVF and Assisted Reproduction After Endometrial Cancer
Assisted reproduction is often the fastest route to pregnancy after conservative therapy, and cryopreservation offers options if immediate surgery is needed.
Spanish fertility clinics are experienced in fast-track preservation and ART pathways for oncology patients.
When IVF is recommended
IVF is usually advised when:
- A patient has achieved complete response and wants to minimize delay before conception
- Underlying infertility factors (e.g., poor ovulation) exist
Egg and embryo freezing options (urgent preservation before definitive treatment)
- Egg or embryo vitrification is recommended before surgery or systemic therapy when time allows.
- If hysterectomy becomes necessary, frozen embryos can enable parenthood via surrogacy where legally permitted.
What Happens After You Complete Pregnancy?
Most specialists recommend definitive hysterectomy once childbearing is finished to reduce long-term recurrence risk. This is an oncologic safety step taken after successful childbearing.
Why doctors often recommend hysterectomy afterward
Because conservative management has a higher long-term risk of recurrence than standard surgery, most clinicians recommend definitive hysterectomy after childbearing is complete. This reduces recurrence risk and aligns with oncologic safety.
Emotional and Psychological Considerations
Balancing cancer treatment with fertility hopes is emotionally intense. Patients often face fear, hope, and difficult trade-offs.
Access to counseling and peer support improves coping and informed decision-making.
Fear, hope, and decision-making
Decisions about fertility vs. cancer control are emotionally fraught. It’s normal to experience grief, guilt, hope and anxiety simultaneously. Clear information, time (when possible), and compassionate counseling help patients make choices they can live with.
Support systems in Spain
Spanish hospitals and private clinics increasingly integrate psycho-oncology, patient navigators and support groups into care. Multilingual teams and experience with international patients can ease legal and logistical concerns surrounding surrogacy or cross-border fertility services.
When Should You Speak to a Specialist?
If you’re diagnosed or suspect endometrial pathology, early specialist input is essential — especially if you wish to preserve fertility.
A timely referral can make the difference between immediate loss of options and coordinated fertility-preserving care.
Red flags and timing
Speak to a gynecologic oncologist and fertility specialist as soon as endometrial hyperplasia or early cancer is suspected—before any irreversible surgery. Early referral preserves options.
Getting a second opinion
A second opinion is often helpful when fertility is a priority. Different centers may have different thresholds and protocols for offering conservative treatment; compare recommendations and ensure the decision is made by an experienced multidisciplinary team.
FAQs
Can you get pregnant with endometrial cancer right now?
Only in very rare situations; typically pregnancy attempts follow a period of conservative treatment and confirmed remission.
How long after conservative treatment should I wait to try to conceive?
Timing varies by protocol, but conception attempts are usually advised after documented complete response and in coordination with a fertility specialist.
Will hormonal therapy for cancer harm my eggs?
Progestin therapy acts mainly on the endometrium and is not directly toxic to eggs; however, if definitive surgery or systemic therapy is needed, egg preservation should be discussed.
Can I freeze eggs if I need immediate hysterectomy?
If there is sufficient time before surgery, egg or embryo freezing is often possible and recommended; discuss urgent preservation with your fertility team.
Is surrogacy allowed for cancer survivors in Spain?
Spanish law restricts surrogacy; many patients consider international surrogacy options and should obtain legal counsel and clinic guidance before pursuing this path.
Conclusion
Yes — in selected, carefully evaluated cases, you can get pregnant with endometrial cancer, but it requires strict selection, close monitoring, and a multidisciplinary plan. Spain’s integrated cancer and fertility services, and clinicians such as Dr. Lucas Minig, provide pathways that balance safety and patient goals. If preserving fertility matters to you, ask your team about fertility-preserving options and fast-track egg/embryo preservation before any irreversible treatment.